
- Popular searches
- Bell & Ross
- Audemar Piguet
- BELL & ROSS

100% Certified Authentic | Two Year International Worry Free Warranty | Free Nationwide Shipping
- AUDEMARS PIGUET
- PATEK PHILIPPE
- MEN'S WATCHES
- WOMEN'S WATCHES

- Sell Your Watch

- Bell & Ross
- Sell Your Rolex
- Sell Your Patek Philippe
- Sell Your Vacheron Constantin
- Sell Your Richard Mille
- Sell Your Audemars Piguet
- Sell Your Breitling
- Sell Your Cartier
- Watch Service
For over 30 years, our family-owned luxury watch store has provided customers with quality products and exceptional service. Our third-generation business is proud to bring you an extensive selection of watches from top Swiss Watch brands. Our team of experts is here to help you find the perfect timepiece that fits your style and budget.
- Discover Rolex
- Rolex watches
- New watches 2024
- Watchmaking
- World of Rolex
- The Yacht-Master collection
- M226627-0001

Oyster, 42 mm, RLX titanium
Water-resistance
Waterproof to 100 metres / 330 feet
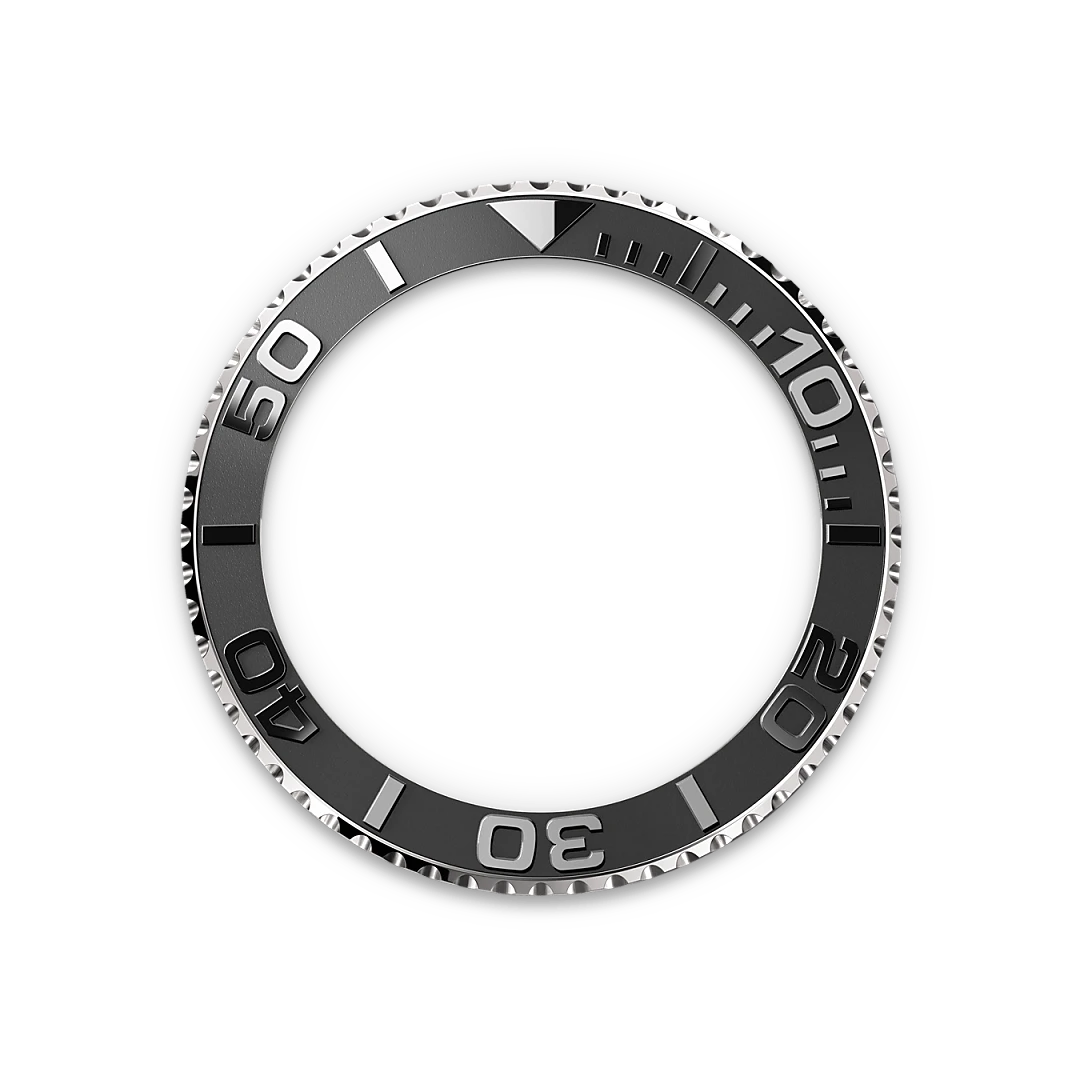
Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations
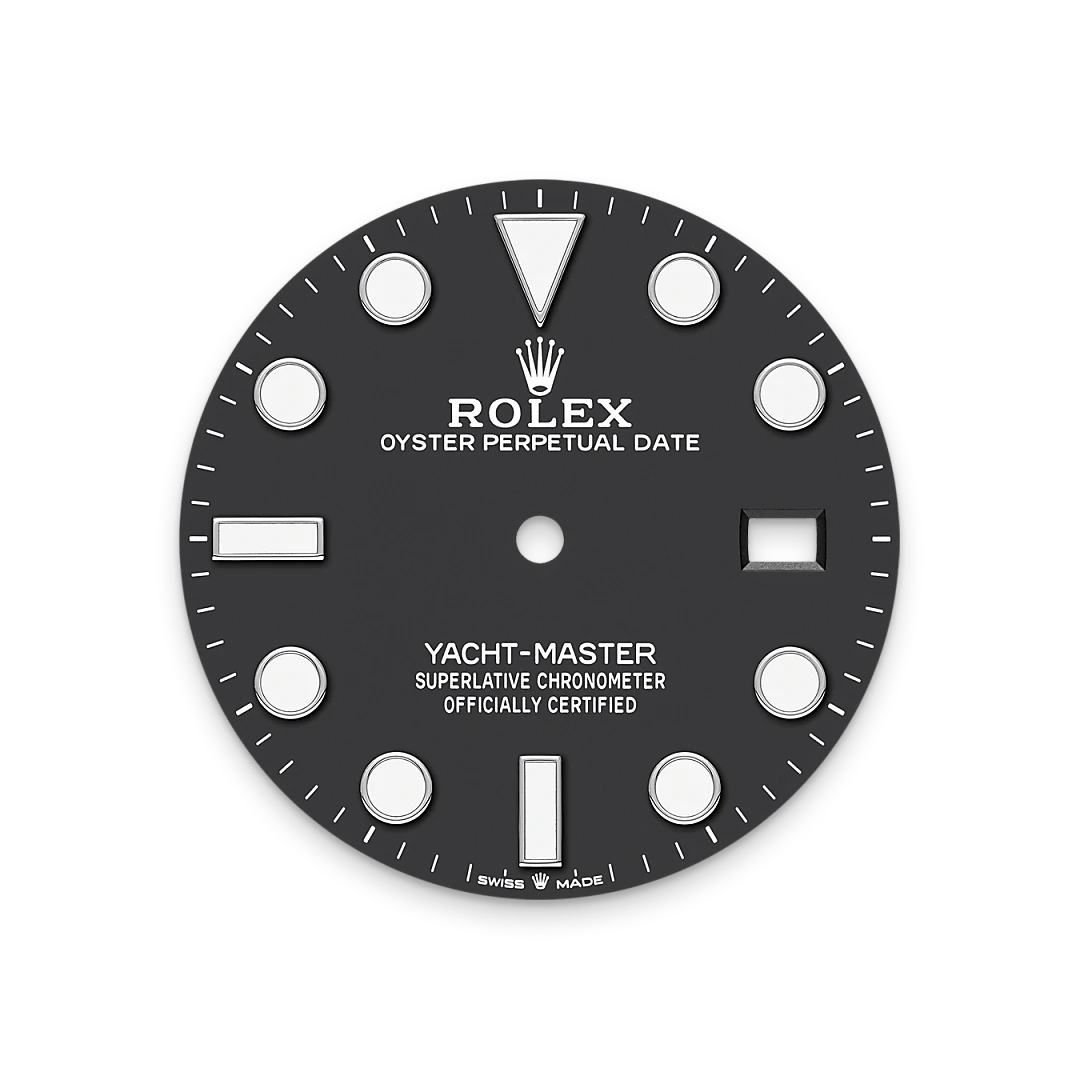
Intense black
Oyster, three-piece solid links
Perpetual, mechanical, self-winding
3235, Manufacture Rolex


Bidirectional Rotatable Bezel
The Yacht-Master’s bidirectional rotatable 60-minute graduated bezel is made entirely from precious metals or fitted with a Cerachrom insert in high-tech ceramic. The raised polished numerals and graduations stand out clearly against a matt, sand-blasted background. This functional bezel – which allows the wearer to calculate, for example, the sailing time between two buoys – is also a key component in the model’s distinctive visual identity.

Intense black dial
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes – triangles, circles, rectangles – are filled with a luminescent material emitting a long-lasting glow.

RLX titanium
RLX titanium is a grade 5 titanium alloy specially selected by Rolex. Like all titanium alloys, it is especially lightweight and is noted for its mechanical strength and corrosion resistance. Another characteristic of RLX titanium is the possibility of working it to give a polished or satin finish according to the brand’s specifications. Its high mechanical strength makes it complex to work with, and the decision to use it has required the introduction of special production processes.

Model availability
All Rolex watches are assembled by hand with the utmost care to ensure exceptional quality. Such high standards naturally restrict Rolex production capacity and, at times, the demand for Rolex watches outpaces this capacity.
Therefore, the availability of certain models may be limited. New Rolex watches are exclusively sold by Official Rolex Retailers, who receive regular deliveries and independently manage the allocation and sales of watches to customers. Precision Watches is proud to be part of the worldwide network of Official Rolex Retailers and can provide information on the availability of Rolex watches.

Please enter your message
Send us a message.
Thank you for your interest in Rolex watches. Please enter your message below and we will be delighted to assist you. Enter your message
Please enter your contact information
Title Mx Mr Ms
+1 +44 +91 +93
Your message
*Mandatory information
*I have read and accepted the terms and conditions and privacy policy.
Your message has been successfully sent to the Rolex team at Precision Watches
One of our Rolex sales advisors will be reviewing your request and responding as soon as possible.

The Watch of the Open Seas
Keep exploring.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish.
Privacy Overview
Welcome to CD Peacock – Chicago’s Premier Jeweler Since 1837

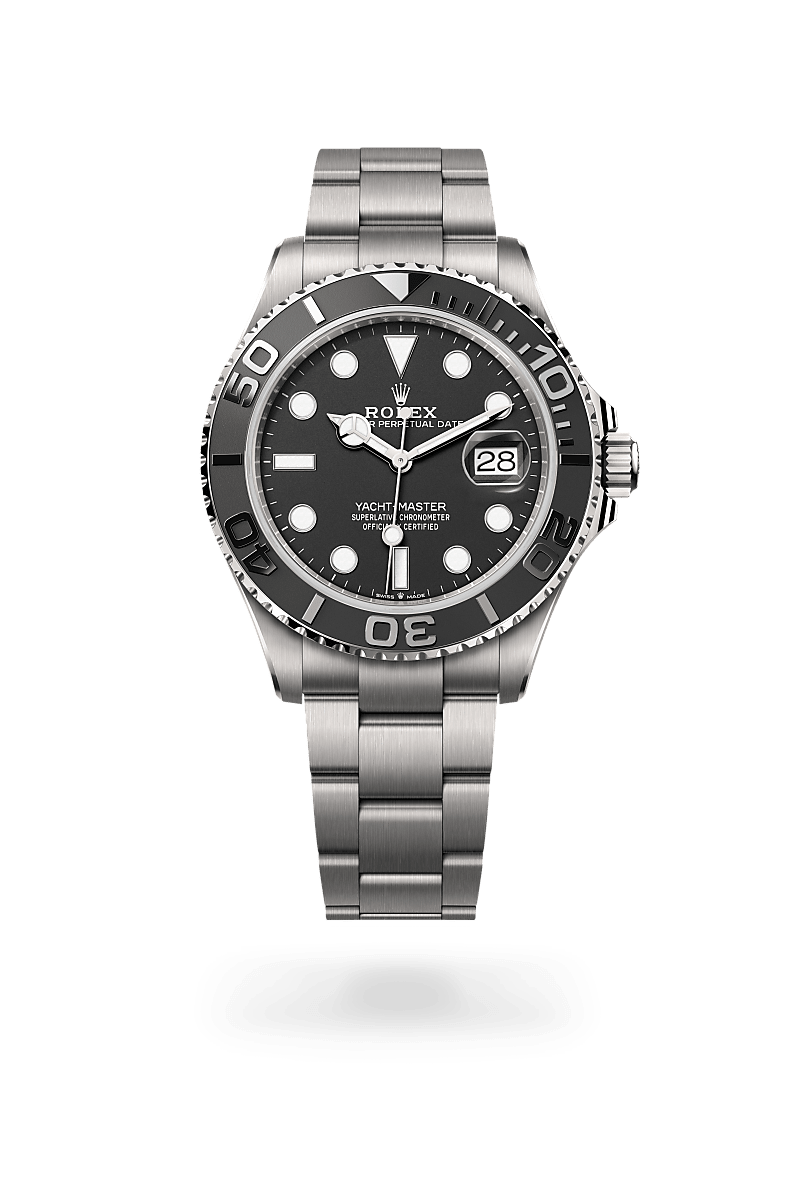
Yacht-Master 42
Oyster, 42 mm, RLX titanium
Water-resistance
Waterproof to 100 metres / 330 feet
Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations
Intense black
Oyster, three-piece solid links
Perpetual, mechanical, self-winding
3235, Manufacture Rolex
Power reserve
Approximately 70 hours
Certification
Superlative Chronometer (COSC + Rolex certification after casing)

Bidirectional Rotatable Bezel
The Yacht-Master’s bidirectional rotatable 60-minute graduated bezel is made entirely from precious metals or fitted with a Cerachrom insert in high-tech ceramic. The raised polished numerals and graduations stand out clearly against a matt, sand-blasted background. This functional bezel – which allows the wearer to calculate, for example, the sailing time between two buoys – is also a key component in the model’s distinctive visual identity.

Intense black dial
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes – triangles, circles, rectangles – are filled with a luminescent material emitting a long-lasting glow.

RLX titanium
RLX titanium is a grade 5 titanium alloy specially selected by Rolex. Like all titanium alloys, it is especially lightweight and is noted for its mechanical strength and corrosion resistance. Another characteristic of RLX titanium is the possibility of working it to give a polished or satin finish according to the brand’s specifications. Its high mechanical strength makes it complex to work with, and the decision to use it has required the introduction of special production processes.

Model availability
All Rolex watches are assembled by hand with the utmost care to ensure exceptional quality. Such high standards naturally restrict Rolex production capacity and, at times, the demand for Rolex watches outpaces this capacity. Therefore, the availability of certain models may be limited. New Rolex watches are exclu-sively sold by Official Rolex Retailers, who receive regular deliveries and independently manage the allocation and sales of watches to customers. C.D.Peacock is proud to be part of the worldwide network of Official Rolex Retailers and can provide information on the availability of Rolex watches.

Send us a message
Please enter your message
Thank you for your interest in Rolex watches. Please enter your message below and we will be delighted to assist you.
Please enter your contact information
I have read and accepted the privacy policy and terms and conditions .

Book an appointment
Please note.
Kindly note that the availability of certain Rolex watches in our point of sale may be tested.
Please select the purpose of your appointment.

Rolex Yacht-Master
Marine character
Description
Related products.

Datejust 41

Explorer 36

Oyster Perpetual 41

Datejust 36

Keep exploring
Discover Rolex

New Watches 2024

Rolex Watches

Watchmaking

- Chicago - 773-327-8800
- Naperville - 630-281-5900
- Orland Park - 708-226-0800
- Schererville - 219-864-9090
Free Shipping on Orders Over $150
Shipping Times & Rates
James & Sons accepts online orders to addresses within the United States only. To ensure the secure delivery of your order, we will not ship to P.O. boxes.
For addresses within the United States, the following charges apply: We are pleased to offer complimentary shipping on all orders over $150. For orders under $150, we offer a flat shipping rate of just $8.00. Please allow 5-7 business days.
Return Policy
Online Return Policy Tudor Watches: All Tudor watches are final sale and not eligible for return.
Rolex Certified Pre-Owned Watches: The return policy for Rolex Certified Pre-Owned watches is 5 business days. Online Rolex Certified Pre-Owned watch purchases are accepted for full refund if returned in new, sell-able condition within 5 days after the date of purchase. Returns must be accompanied by the original sales invoice along with any certificate, packaging, or gift.
Jewelry: If, for some reason, you are not happy with your jewelry purchase, James & Sons offers complimentary shipping for any item that you would like to return. A return shipping label is included in your package. Simply place that label on the outside of your box, ensure that it's secured, and then drop it off at the nearest FedEx location. Online jewelry purchases are accepted for full refund if returned in new, sell-able condition within 30 days after the date of purchase. Returns must be accompanied by the original sales invoice along with any certificate, packaging, or gift.
General Information: Once we receive your returned item and it is accepted, your refund or exchange will be processed. Upon receiving your return, the item and collateral material will be reviewed by our Inventory Department. Please note that items showing signs of wear or those that have been altered, resized or damaged in any way cannot be accepted for return. Special ordered or custom made items, and resized or engraved items may not be returned. We will credit your original method of payment excluding shipping charges within 2 weeks of receiving your return. Please make sure to securely package and fully insure any returns along with original sales invoice and packaging materials. Return packages that are improperly packaged or uninsured will not be accepted. We are not responsible for loss or damage of return shipments in Transit. Please make sure to include your Reason for Return. You also have the option to return your item at any of our retail stores. To see our location information, click here .
Rolex watches
- The Yacht-Master collection
- M226627-0001
Rolex Yacht-Master 42 Oyster, 42 mm, RLX titanium M226627-0001
Yacht-master 42.
42 mm, RLX titanium
$14,050 i All prices are Rolex’s suggested retail price before applicable taxes. Prices can be modified at any time without notice.

Oyster, 42 mm, RLX titanium
Water-resistance
Waterproof to 100 metres / 330 feet
Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations
Intense black
Oyster, three-piece solid links
Perpetual, mechanical, self-winding
3235, Manufacture Rolex
Power reserve
Approximately 70 hours
Certification
Superlative Chronometer (COSC + Rolex certification after casing)

Bidirectional Rotatable Bezel
The Yacht-Master’s bidirectional rotatable 60-minute graduated bezel is made entirely from precious metals or fitted with a Cerachrom insert in high-tech ceramic. The raised polished numerals and graduations stand out clearly against a matt, sand-blasted background. This functional bezel – which allows the wearer to calculate, for example, the sailing time between two buoys – is also a key component in the model’s distinctive visual identity.
Intense black dial
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes – triangles, circles, rectangles – are filled with a luminescent material emitting a long-lasting glow.
RLX titanium
RLX titanium is a grade 5 titanium alloy specially selected by Rolex. Like all titanium alloys, it is especially lightweight and is noted for its mechanical strength and corrosion resistance. Another characteristic of RLX titanium is the possibility of working it to give a polished or satin finish according to the brand’s specifications. Its high mechanical strength makes it complex to work with, and the decision to use it has required the introduction of special production processes.
Model availability
All Rolex watches are assembled by hand with the utmost care to ensure exceptional quality. Such high standards naturally restrict Rolex production capacity and, at times, the demand for Rolex watches outpaces this capacity.
Therefore, the availability of certain models may be limited. New Rolex watches are exclusively sold by Official Rolex Jewelers, who receive regular deliveries and independently manage the allocation and sales of watches to customers.
James & Sons is proud to be part of the worldwide network of Official Rolex Jewelers and can provide information on the availability of Rolex watches.
Marine character
Keep exploring.
Discover Rolex
New watches 2024
Watchmaking
World of Rolex
By clicking "Accept All", you agree to the storing of cookies on your device to enhance site navigation, analyze site usage, and assist in our marketing efforts. You may change your settings at any time or accept the default settings. Cookie Policy Do Not Sell My Personal Information
We value your privacy
On our website, we use services (including from third-party providers) that help us to improve our online presence. The following categories of cookies are used by us and can be managed in the cookie settings. We need your consent before being able to use these services. Alternatively, you may click to refuse to consent, of access more detailed information and change your preferences before consenting. Your preferences will apply to this website only. You can change your preferences at any time by returning to this site or visit our privacy policy.
By authorizing third-party services, you allow the placement and the reading of cookies and the use of tracking technologies required to keep our website reliable and secure.
These cookies are required to run available services and to provide basic shopping functions. These cookies are exempt from consent according to the exceptions provided by the Article 82 of Data Protection Act
| Name: amp_16a5c8 |
| Name: PHPSESSID |
| Name: rlx-consent |
| Name: cmp_cookies |
These cookies provide a custom experience on our website
These cookies allow us to measure visitors traffic. They also help us understand which products and actions are more popular than others
| Name: _gcl_au |
| Name: _fbp |
| Name: _ga_5QGS0HV0QW |
| Name: _ga |
| Name: _gid |
Privacy Policy: https://www.rolex.com/legal-notices/cookies.html
Purposes (consent)
Legimate Interest Purpose(s)
| Name: AMCVS_1FE034B8527850350A490D44%40AdobeOrg |
| Name: s_cc |
| Name: AMCV_1FE034B8527850350A490D44%40AdobeOrg |
| Name: s_sq |
Ben Bridge Jeweler will ship merchandise to United States addresses, United States P.O. Box, US Embassy / Military APO or FPO addresses. We cannot ship international orders at this time.
Item Return Policy
Ben Bridge is committed to ensure our customers are happy with their purchase or gifts. If you have any questions or concerns about our refund policy, please contact your local Ben Bridge store or send us an e-mail.
- Create Account
- Check Order Status

Rolex Yacht-Master 42 Oyster, 42 mm, RLX titanium M226627-0001

All Rolex watches are assembled by hand with the utmost care to ensure exceptional quality. Such high standards naturally restrict Rolex production capacity and, at times, the demand for Rolex watches outpaces this capacity.
Therefore, the availability of certain models may be limited. New Rolex watches are exclusively sold by Official Rolex Jewelers, who receive regular deliveries and independently manage the allocation and sales of watches to customers.
Ben Bridge is proud to be part of the worldwide network of Official Rolex Jewelers and can provide information on the availability of Rolex watches.

Send a message
Please enter your message
Thank you for your interest in Rolex watches. Please enter your message below and we will be delighted to assist you.
Please enter your contact information

Discover Rolex

Rolex watches

New watches 2024

Watchmaking

World of Rolex

Your message has been sent. We will contact you shortly.
Added to Manage List
Removed from Undo
List Updated Manage List
JavaScript seems to be disabled in your browser. You must have JavaScript enabled in your browser to utilize the functionality of this website.
- (954) 782-5000
Rolex YACHT-MASTER Oyster, 42 mm, RLX titanium M226627-0001
Yacht-master 42.
Oyster, 42 mm, RLX titanium
+1 954-710-5742
Model availability
Water-resistance
Waterproof to 100 metres / 330 feet
Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations
Intense black
Oyster, three-piece solid links
Perpetual, mechanical, self-winding
3235, Manufacture Rolex
Power reserve
Approximately 70 hours
Certification
Superlative Chronometer (COSC + Rolex certification after casing)
Bidirectional Rotatable Bezel
The Yacht-Master's bidirectional rotatable 60-minute graduated bezel is made entirely from precious metals or fitted with a Cerachrom insert in high-tech ceramic. The raised polished numerals and graduations stand out clearly against a matt, sand-blasted background. This functional bezel - which allows the wearer to calculate, for example, the sailing time between two buoys - is also a key component in the model's distinctive visual identity.
Intense black dial
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes - triangles, circles, rectangles - are filled with a luminescent material emitting a long-lasting glow.
RLX titanium
RLX titanium is a grade 5 titanium alloy specially selected by Rolex. Like all titanium alloys, it is especially lightweight and is noted for its mechanical strength and corrosion resistance. Another characteristic of RLX titanium is the possibility of working it to give a polished or satin finish according to the brand's specifications. Its high mechanical strength makes it complex to work with, and the decision to use it has required the introduction of special production processes.
All Rolex watches are assembled by hand with the utmost care to ensure exceptional quality. Such high standards naturally restrict Rolex production capacity and, at times, the demand for Rolex watches outpaces this capacity.
Therefore, the availability of certain models may be limited. New Rolex watches are exclusively sold by Official Rolex Jewelers, who receive regular deliveries and independently manage the allocation and sales of watches to customers. J.R. Dunn is proud to be part of the worldwide network of Official Rolex Jewelers and can provide information on the availability of Rolex watches.
Send us a message
Send a message
Please enter your message.
Thank you for your interest in Rolex watches. Please enter your message below and we will be delighted to assist you.
Please enter your contact information
Your message has been successfully sent to the Rolex team at J.R. Dunn
One of our Rolex sales advisors will be reviewing your request and responding as soon as possible.
Rolex Yacht-Master
Marine character, keep exploring.

Visit us in real life.
Meet our team, store location.
- Mon-Sat: 10am — 6pm
- Sunday: Closed
Save up to 15% on your first order.
Have no fear, we’ll email this code to you also!
Philanthropy
First responders, privacy policy, terms of use, cookie preferences.
Sorry! Something went wrong with your cart. Go to full cart and try again?
Oops! Something is wrong on our end. Call 888.969.3501 or text “AFTERHOURS” to 833.222.2658 and we’ll work our magic!
Watch Battery Month Benefitting Children’s Cancer Research Fund: We’re donating 100% of watch battery sales in September to improve the lives of kids fighting cancer.
No products in the cart.

- Discover Rolex
- Rolex Watches
- New Watches 2024
- Watchmaking
- World of Rolex
- Rolex at R.F. Moeller Jeweler
- Contact Us
- Yacht-Master
- M226627-0001
Rolex Yacht-Master 42 Oyster, 42 mm, RLX titanium $14,050 All prices are Rolex's suggested retail price before applicable taxes. The suggested price can be modified at any time without notice. -->
- Reference 226627
- Model Case Oyster, 42 mm, RLX titanium
- Bezel Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations
- Water-Resistance Waterproof to 100 metres / 330 feet
- Movement Perpetual, mechanical, self-winding
- Calibre 3235, Manufacture Rolex
- Power-Reserve Approximately 70 hours
- Bracelet Oyster, three-piece solid links
- Dial Intense black
- Certification Superlative Chronometer (COSC + Rolex certification after casing)
The Yacht-Master’s bidirectional rotatable 60-minute graduated bezel is made entirely from precious metals or fitted with a Cerachrom insert in high-tech ceramic. The raised polished numerals and graduations stand out clearly against a matt, sand-blasted background. This functional bezel – which allows the wearer to calculate, for example, the sailing time between two buoys – is also a key component in the model’s distinctive visual identity.
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes – triangles, circles, rectangles – are filled with a luminescent material emitting a long-lasting glow.
RLX titanium is a grade 5 titanium alloy specially selected by Rolex. Like all titanium alloys, it is especially lightweight and is noted for its mechanical strength and corrosion resistance. Another characteristic of RLX titanium is the possibility of working it to give a polished or satin finish according to the brand’s specifications. Its high mechanical strength makes it complex to work with, and the decision to use it has required the introduction of special production processes.

Model Availability
All Rolex watches are assembled by hand with the utmost care to ensure exceptional quality. Such high standards naturally restrict Rolex production capacity and, at times, the demand for Rolex watches outpaces this capacity.
Therefore, the availability of certain models may be limited. New Rolex watches are exclusively sold by Official Rolex Jewelers, who receive regular deliveries and independently manage the allocation and sales of watches to customers. R.F. Moeller Jeweler is proud to be part of the worldwide network of Official Rolex Jewelers and can provide information on the availability of Rolex watches.

Send a message
Please enter your message
Thank you for your interest in Rolex watches. Please enter your message below and we will be delighted to assist you.
" * " indicates required fields

Rolex Yacht-Master
Marine character
Keep exploring.
- Rolex Collection
- Servicing Your Rolex
- Our Rolex Team
- Our Rolex Showrooms
- Our History
.css-1c7en8u{font-size:clamp(1.375rem, 1.25rem + 0.3125vw, 3.125rem);line-height:1.1;margin-bottom:1rem;} Yacht-Master 42 .css-1g7r01k{font-weight:300;font-size:clamp(0.875rem, 0.9375rem + 0.1563vw, 1.25rem);line-height:1.2;text-wrap:balance;}.css-1g7r01k span{display:block;} Oyster, 42 mm, white gold Reference 226659
View in night mode
Discover in 360°
Staying on course
The Oyster Perpetual Yacht-Master 42 in 18 ct white gold with a black dial and an Oysterflex bracelet.
The oysterflex bracelet, highly resistant and durable.
The Yacht-Master’s new Oysterflex bracelet, developed by Rolex and patented, offers a sporty alternative to metal bracelets. The bracelet attaches to the watch case and the Oysterlock safety clasp by a flexible titanium and nickel alloy metal blade.
The blade is overmoulded with high-performance black elastomer which is particularly resistant to environmental effects, very durable and perfectly inert for the wearer of the watch. For enhanced comfort, the inside of the Oysterflex bracelet is equipped with a patented longitudinal cushion system that stabilizes the watch on the wrist and fitted with an 18 ct white gold Oysterlock safety clasp. It also features the Rolex Glidelock extension system, designed by the brand and patented. This inventive toothed mechanism, integrated beneath the clasp, allows fine adjustment of the bracelet length by some 15 mm in increments of approximately 2.5 mm, without the use of tools.
18 ct white gold
Commitment to excellence
By operating its own exclusive foundry, Rolex has the unrivalled ability to cast the highest quality 18 ct gold alloys. According to the proportion of silver, copper, platinum or palladium added, different types of 18 ct gold are obtained: yellow, pink or white.
They are made with only the purest metals and meticulously inspected in an in-house laboratory with state-of-the-art equipment, before the gold is formed and shaped with the same painstaking attention to quality. Rolex's commitment to excellence begins at the source.
Bidirectional Rotatable Bezel
Timing the distance.
The Yacht-Master’s bidirectional rotatable 60-minute graduated bezel is made entirely from precious metals or fitted with a Cerachrom insert in high-tech ceramic. The raised polished numerals and graduations stand out clearly against a matt, sand-blasted background.
This functional bezel – which allows the wearer to calculate, for example, the sailing time between two buoys – is also a key component in the model’s distinctive visual identity.
Exceptional legibility
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display.
The broad hands and hour markers in simple shapes – triangles, circles, rectangles – are filled with a luminescent material emitting a long-lasting glow.
More Yacht-Master technical details
Reference 226659
Model case .css-plfq1t{--iconSize:12px;--iconStrokeWidth:2px;height:var(--iconSize);position:relative;width:var(--iconSize);}.css-plfq1t::before,.css-plfq1t::after{background:currentColor;content:"";display:block;height:var(--iconStrokeWidth);left:0;position:absolute;right:0;top:50%;-webkit-transition:-webkit-transform 0.6s;transition:transform 0.6s;will-change:transform;}html.prefers-reduced-motion .css-plfq1t::before,html.prefers-reduced-motion .css-plfq1t::after{-webkit-transition:none;transition:none;}.css-160voq8 .css-plfq1t::after{-webkit-transform:rotate(90deg);-moz-transform:rotate(90deg);-ms-transform:rotate(90deg);transform:rotate(90deg);}.no-js .css-plfq1t{display:none;}
Oyster, 42 mm, white gold
Oyster architecture
Monobloc middle case, screw-down case back and winding crown
Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations
Winding crown
Screw-down, Triplock triple waterproofness system
Scratch-resistant sapphire, Cyclops lens over the date
Water resistance
Waterproof to 100 metres / 330 feet
Perpetual, mechanical, self-winding
3235, Manufacture Rolex
-2/+2 sec/day, after casing
Centre hour, minute and seconds hands. Instantaneous date with rapid setting. Stop-seconds for precise time setting
Paramagnetic blue Parachrom hairspring. High-performance Paraflex shock absorbers
Bidirectional self-winding via Perpetual rotor
Power reserve
Approximately 70 hours
Flexible metal blades overmoulded with high-performance elastomer
Folding Oysterlock safety clasp with Rolex Glidelock extension system
Highly legible Chromalight display with long-lasting blue luminescence
Certification
Superlative Chronometer (COSC + Rolex certification after casing)
Learn how to set the time and other functions of your Rolex watch by consulting our user guides.
Yacht-Master 42
Contact an Official Rolex Retailer
Only official Rolex retailers are allowed to sell and maintain a Rolex watch. With the necessary skills, technical know-how and special equipment, they guarantee the authenticity of each and every part of your Rolex and help you make the choice that will last a lifetime.
Watches you may like
These watches have been selected for you. Add them with the heart icon to your favorites.

Rolex Yacht-Master 42 Black Dial Titanium Men's Watch 226627-0001

You May Also Like

Subscribe to our mailing list
Join the wait list.
- Hours & Locations
- Cosmograph Daytona
- GMT-Master II
- Lady Date-Just
- Oyster Perpetual
- Sea-Dweller
- Sky-Dweller
- Yacht-Master
- Rolex Watches
- Rolex Watchmaking
- Servicing Your Rolex
- Rolex Servicing Procedure
- World of Rolex
- Our Rolex Showroom
- Our Rolex History
- Our Rolex Team
- New watches 2024
- New Designs
- Necklaces & Chains
- Accessories
- The Cable Collection®
- Gold Plain Chains
- The Crossover® Collection
- Châtelaine®
- DY Elements
- Streamline®
- Engagement Rings
- Wedding Rings
- Diamond Bands
- Classic Bands
- Alternative Bands
- Mountings & Semi Mounts
- Ladies Diamond Bands
- Anniversary Rings

- David Yurman
- Necklaces & Pendants
- Roberto Coin
- Leonardo Collection
- Temple St. Clair
- Marco Bicego
- Hulchi Belluni
- Alex Sepkus
- Annamaria Cammilli
- Matthia's and Claire
- Melissa Kaye
- Doves by Doron Paloma
- Platinum Born
- Serafino Consoli
- Sasha Primak

- Grand Seiko
- IWC Schaffhausen
- Ulysse Nardin
- Watch Winders
- Watch Storage

- Watch Repair
- Jewelry Repair
- Jewelry Insurance

- William Henry
- Why Choose Us?
- Contact Us & Hours
- Testimonials

We value your privacy
On our website, we use services (including from third-party providers) that help us to improve our online presence. The following categories of cookies are used by us and can be managed in the cookie settings. We need your consent before being able to use these services. Alternatively, you may click to refuse to consent, or access more detailed information and change your preferences before consenting. Your preferences will apply to this website only. You can change your preferences at any time by clearing your browser history/cache or visiting our privacy policy page.
By authorizing third-party services, you allow the placement and the reading of cookies and the use of tracking technologies required to keep our website reliable and secure.
Review and set your consent preferences for each partner below. Some personal data is processed without your consent, but you have the right to object.
Rolex (Adobe Analytics and Content Square)
Privacy policy: https://www.rolex.com/legal-notices/cookies.html Purposes (consent) Legitimate interest Purpose(S)
We are using cookies to give you the best experience on our website.
You can find out more about which cookies we are using or switch them off in settings.
- Rolex watches
- M226627-0001
Yacht-Master 42
Oyster, 42 mm, RLX titanium
All prices are Rolex's suggested retail price before applicable taxes. Prices can be modified at any time without notice.

- Reference 226627
- Model case Oyster, 42 mm, RLX titanium
- Water-resistance Waterproof to 100 metres / 330 feet
- Bezel Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations
- Dial Intense black
- Bracelet Oyster, three-piece solid links
- Movement Perpetual, mechanical, self-winding
- Caliber 3235, Manufacture Rolex
- Power reserve Approximately 70 hours
- Certification Superlative Chronometer (COSC + Rolex certification after casing)

Bidirectional Rotatable Bezel
The Yacht-Master’s bidirectional rotatable 60-minute graduated bezel is made entirely from precious metals or fitted with a Cerachrom insert in high-tech ceramic. The raised polished numerals and graduations stand out clearly against a matt, sand-blasted background. This functional bezel - which allows the wearer to calculate, for example, the sailing time between two buoys - is also a key component in the model’s distinctive visual identity.

Intense black dial
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes - triangles, circles, rectangles - are filled with a luminescent material emitting a long-lasting glow.

RLX titanium
RLX titanium is a grade 5 titanium alloy specially selected by Rolex. Like all titanium alloys, it is especially lightweight and is noted for its mechanical strength and corrosion resistance. Another characteristic of RLX titanium is the possibility of working it to give a polished or satin finish according to the brand’s specifications. Its high mechanical strength makes it complex to work with, and the decision to use it has required the introduction of special production processes.

Model availability

Marine character
Keep exploring.

Come by Our Store
1155 Connecticut Ave, NW Washington, DC 20036
Monday - Saturday 10AM - 5.30PM Sunday: Closed
PARKING VALIDATION
Monday – Friday: Colonial Parking 1140 Connecticut Ave, NW (Closes at 3pm daily)
Saturday: PMI Parking [ 1725 Desales St, NW ]
Request Product Information
university of reading creative writing

- business plan
- course work
- research paper
case study of bad teamwork

Work Life is Atlassian’s flagship publication dedicated to unleashing the potential of every team through real-life advice, inspiring stories, and thoughtful perspectives from leaders around the world.

Contributing Writer

Work Futurist

Senior Quantitative Researcher, People Insights

Principal Writer

How 6 seasoned managers tackle the biggest challenges of teamwork
Detect, resolve, and prevent common problems that can derail your team
5-second summary
- Teamwork is essential for success no matter what industry you’re in, but it can be derailed in a number of different ways.
- Connecting the dots between what your team is doing and why they’re doing it goes a long way in addressing (and preventing) many of the most common teamwork challenges.
- Taking the time to listen to team members’ hopes and concerns builds a better working relationship, which makes any of these challenges easier to overcome.
Whoever said “teamwork makes the dream work” may have been onto something. That doesn’t mean it’s always smooth sailing, though. If your team has struggled with unclear goals, low engagement, or personality conflicts, then you know how quickly the dream can turn into a nightmare.
Teams at Atlassian are no strangers to the challenges of teamwork, and we’re always keen to share what has worked for us and what hasn’t. So I called up a handful of my esteemed colleagues to learn more about some of the most prevalent challenges. I asked them how to know when your team is struggling (it’s not always obvious!), what to do about it, and how to prevent the problem in the first place. Here’s what they said.
Get stories like this in your inbox
Challenge #1: low engagement
Highly engaged teams tend to do better when it comes to devising solutions to gnarly problems and hitting their goals on time. But as many as 53 percent of workers were disengaged to some extent even in pre-pandemic times. Now, between the additional stress many people are still feeling and the fact that fewer teams are sharing physical office space, that number is likely to be even higher.
Warning signs
“If your team-wide Slack channels have gone silent and checking off tasks has started to feel like pulling teeth, engagement levels could be slipping,” says Sarah Larson, Atlassian’s head of talent. Other signs of low engagement include resistance to change, a decline in the quality or timeliness of work, and general complacency. If members of your team who used to be excited and communicative are suddenly distant and only willing to do the bare minimum, something is up.
What to do about it
To bring your team back into the fold, Sarah recommends two tactics. First, connect with your team members individually through regular 1-on-1s. Rather than discussing project updates, ask how they’re feeling about their work and how you can support them. And don’t forget to praise their accomplishments. “Even a small token of appreciation like a coffee or a shoutout over Slack can go a long way toward inspiring great work,” she says.
Second, make sure they understand how their work contributes to the bigger picture. “Draw a clear line between a task or project and the broader company goal it supports,” Sarah says. And, she cautions, “If you can’t identify a connection, ask yourself if that task actually needs to be done.”
She also recommends sharing customer quotes or stories that may help the team see the impact of their work and initiating cross-functional projects so they better understand where their piece fits into the puzzle.
How to prevent it
As for keeping engagement high, the best way to check on your team’s motivation levels is to ask. It could be through a quarterly company-wide survey, a casual check-in during one-on-ones, or anything in between.
You can also take a page from best-selling author Dan Pink’s playbook: create an environment where people have a strong sense of purpose, opportunities to master their craft, and the autonomy to make day-to-day decisions about their work. Autonomy + mastery + purpose = intrinsic motivation. And intrinsic motivation beats the carrot-and-stick variety any day of the week.
Control leads to compliance, autonomy leads to engagement. – Dan Pink, Drive: The Surprising Truth About What Motivates Us
Challenge #2: lack of trust
When you join or form a new team, trust is neutral: there is neither trust nor distrust. Your first few interactions determine whether you move upward toward trust, or downward toward distrust. So it’s up to leaders to create an environment that inspires upward movement, according to Atlassian’s resident work futurist, Dom Price.
Trust is a tricky one because the signs of a low-trust team can be counterintuitive. A non-stop parade of high-fives all around could be a facade.
“Look for the extremes,” he says. “If everyone is smiling all the time, they’re probably not being authentic. Similarly, if everyone is downcast, quiet, resigned to failure, and just going through the motions, that’s bad, too.”
You’ve probably been advised to show empathy, vulnerability, and authenticity if you want to foster trust throughout your team. And you should. (One manager shares 17 ways to do that, here .) That flavor of trust-building takes time and patience, though. So which tactics can you use to increase trust today?
“The cognitive science on building belonging and trust between teammates is all about clarity,” Dom says. “What’s our mission, what do I contribute to the team, what’s expected of me in terms of how we work together?” He advises managers to answer those questions first. That’s your team’s social contract . Then, make sure you hold everyone accountable. The less deviation from that contract, the more trust they’ll have in one another.
Use this Roles and Responsibilities exercise from the Atlassian Team Playbook to clarify all of the above in just one hour. And for a deep-dive on team culture and expectation, add the Working Agreements play.
To prevent trust issues from popping up or recurring, strive to create an atmosphere of connection and belonging. The magic ingredient here is time. “We’ve accidentally become quite transactional in our relationships,” Dom notes. “But spending time getting to know each other personally is what builds team cohesion and genuine bonds.” Even if it’s just a few minutes of small talk at the beginning of meetings.

5 employee engagement ideas that build authentic connections
When you see teammates sharing opposing opinions in a way that doesn’t alienate the other person and without fear that it’s going to get them fired, you’re on the right track. Dom also recommends using the Health Monitor technique he pioneered at Atlassian to keep tabs on team sentiment and spot emerging issues before they flare into bona fide problems.
Challenge #3: information silos
Within the context of a single team or department, people might hoard knowledge in an effort to gain an advantage over their peers or because they think it’s the path to job security. But just as often, it’s simple carelessness. In my 20-odd years in the workforce, I’ve seen countless examples of how information sharing can go by the wayside when you’re cranking through your day-to-day.
If you’re noticing tension and infighting on your team, there’s a good chance an information silo is lurking somewhere under the surface. Duplicated effort is another sign to watch for – when you don’t know what others are up to, or what’s been tried in the past, you often reinvent the wheel.
As a leader, you have at least two roles to play. First, be a model of transparency. Ask your team members and peers for feedback on a piece of work that’s still in progress. Make every Word doc, Confluence page , and Google doc you create open and discoverable (unless there’s a legal reason to lock it down). Change the settings on your calendar to show exactly what’s on your schedule by default, instead of just showing you’re “busy.”
Second, be a cheerleader for things that were successful because people collaborated openly. Did you save 30 minutes of asking around because you were able to find the information you needed on your own? Give a public shout-out to the person who made that possible.
Your third role might be mediator and/or peace-maker, depending on why the silo exists. See above, re: building trust.
Over my many years of working with multiple teams, I’ve noticed that making sure people feel valued in their roles goes a long way in preventing information silos. When your place in the world is secure, you’re more open and less competitive (or at least less nasty in your competitiveness). Of course, tools for sharing information are critical in our digital-first world. The key is configuring them to make information open by default so it’s easy to discover.
Challenge #4: short-term thinking
Obviously, you need short-term, tactical thinking some of the time. But unless your team pursues tactics in the service of a larger goal, they’ll chase a lot of “ shiny objects ” and won’t have much to show for it.
David Turnquist is Atlassian’s head of business strategy and operations, focusing on long-term strategy. According to him, a healthy team should be able to articulate their long-term goal or North Star. “For example,” he says, “when your team is kicking off a new project, ask them about their rationale. If they’re a long-term thinking team, they’ll be connecting the project back to their longer-term goals.” If they can’t, that’s a problem.
Another clue, especially for organizations that are growing quickly, is whether the team frames their strategies in terms of the way things are today or the way things might be a few years from now – like a hockey player skating to where the puck is going to be. Last, David recommends looking at the team’s attitude toward change. Teams that are a bit too in love with the status quo are often ignoring long-term possibilities.
To help them get out of this rut, remind your team of your long-term objectives are at every opportunity. “A good case study here is Atlassian’s goal of getting all our customers migrated over to our cloud products,” David says. “We had TV screens in every office scrolling past migration stats, slogans, etc. Plus, [co-CEOs] Mike and Scott would talk about migration in every single all-hands meeting.” Don’t forget to challenge your team to make their case for new project ideas in a way that connects with their long-term goals, too. If they can’t, push them to re-shape the idea such that it does.
Focusing on the “why” is also a great prevention technique. David and his team periodically review all their projects in the context of their long-term goals. “Sometimes your goals or the shape of your project shifts and it’s easy to get a little off track,” he notes. “If you consistently ask yourself how it all fits into your current understanding of your goals, it reminds people to think long-term and prompts you to refocus your projects so they stay relevant.”
He also advises managers to create time for their team to do some open-ended, blue-sky thinking. Feeling like you’re stuck on a treadmill of small tasks can lead your brain into short-term mode. Dreaming up your “next big thing” helps stop that from happening.

3 signs your team doesn’t have an ownership mindset and what to do about it
Challenge #5: unclear goals.
Speaking of big, blue-sky big objectives, your organization probably has a handful of these, set at the company or department level. At Atlassian, we expect roughly 60 percent of each teams’ work to ladder up to those big goals, according to Ron Romain, a senior program manager. That doesn’t mean the other 40 percent should be scattered in all directions, but… well, sometimes that’s exactly what happens.
“We do occasionally see teams jumping from project to project without ever stopping to ask whether they actually accomplished whatever they hoped to do,” he admits. That’s a dead giveaway that the team was never clear on why they did the work in the first place.
Another red flag is when people are optimizing for different things. Cross-functional project teams are especially prone to this. As a writer, I might optimize for clarity and readability when crafting copy for a marketing campaign. But for the strategist leading the campaign, messaging and product positioning might be the top priority. If we don’t have a shared understanding of our goal, we’ll butt heads and make a mess of the whole thing (and damage our working relationships in the process).
If this sounds like your team, the best way to remedy the situation is to pause your work and get on the same page. “A lot of times, managers hesitate to slow things down,” Ron says. “But if you’re working on the wrong things, that’s far more damaging than taking half a day to run an alignment workshop and build a shared understanding of the goal you’re pursuing.” Be sure to include exercises like Trade-off Sliders that help your team agree on what to optimize for in a given project.
To avoid confusion around goals, use a structured goal-setting framework. Although Ron is a big fan of the OKR method we use at Atlassian, he says KPIs , BHAGs , and SMART goals may work just as well, depending on the team. (Who’s hungry for alphabet soup?) “The key is setting those objectives, then holding yourselves accountable to them,” he cautions. “If you don’t keep those goals front and center, you’ll end up working on too many projects that don’t align to them.”
Challenge #6: personality conflicts
Whether it’s a specific dispute or ongoing low-grade animosity, nothing kills a team’s mojo faster than personality conflicts.
The vibe becomes tense. Debates heat up quickly. And in some cases, you might see a spike in absenteeism or notice that a team member has a sudden and unexplained tendency to decline meetings.
“The verbal and non-verbal cues are always a good indicator,” says Susan Kelbaugh, an employee relations manager at Atlassian. Teammates taking a snarky tone with each other in meetings or making a show of ignoring a colleague when they’re speaking are pretty clear signs. If you’re having trouble pinpointing the source of the problem, she also recommends checking in with team members one-on-one as to how they feel about the team.
While personality conflicts are often easy to detect, resolving them can be a difficult matter that requires patience and good faith on all sides. Susan advises the manager to be direct, but delicate. “Addressing it head-on with the employees involved is always good,” she says. “Listen and repeat back your understanding of what the issue is. Then brainstorm potential fixes with them to ensure the issue doesn’t continue.”
She encourages leaders to speak with team members individually so the conversation doesn’t devolve into finger-pointing. Kick off the discussion by clarifying that your intention is to help the team work better together – not to demonize any one person. As you’re listening, be open to any feedback they might have about the team’s culture, structure, or processes. A small change might pave the way to team harmony.
If your organization has an employee relations specialist, take advantage of their expertise. They can help both managers and employees navigate conflicts so nobody feels alone. The earlier you pull them in, the better.
When you’re bringing in someone new from outside, including current team members in the interview process helps weed out (or at least identify) candidates who are likely to clash with the existing team. Even when a new member is coming from inside the org, Susan suggests setting them up with an onboarding buddy and doing a few team-building activities. This can help them connect with their teammates on a personal level and get a deeper sense of where others are coming from.
We’ve also found that interviewing for values alignment helps build teams that share fundamental attitudes about work and collaboration, while still allowing for diverse backgrounds, skills, and ways of thinking. There’s no guaranteed way to prevent personality clashes, but with a few tweaks to your hiring practices and investment in building personal relationships, you can get pretty close.
Advice, stories, and expertise about work life today.

Examples of Good Team Dynamics and Bad Team Dynamics to Look Out For as a Leader
Learn to recognize the sign of effective team dynamics (as well as negative team dynamics) and start taking steps to improve your team's performance today., recognize your team's dynamics and improve its performance.
📥 Want to turn these insights into action? Download this FREE team building resource!
TeamVitals Team Health Score

What are examples of effective team dynamics? Good team dynamics include open communication, clear expectations, and mutual trust, leading to increased productivity and employee satisfaction. In contrast, bad team dynamics involve poor communication, unresolved conflicts, and a lack of collaboration, resulting in decreased efficiency and higher employee turnover. Recognizing and addressing these dynamics can transform a team's performance. Fostering a healthy work environment is essential for organizational success.
Looking for a baseline of your team's chemistry? Consider trying TeamDynamics , the only personality test built for modern teams.
In this article:
Team dynamics are the unspoken rules and interpersonal interactions that drive a team's performance . That means that the dynamics of a team determine how people communicate, make decisions, and work together towards common goals. Good team dynamics can lead to high productivity, creativity, and innovation in the workplace. Bad team dynamics can lead to dysfunction, conflict, and missed deadlines. In today's fast-paced and competitive workplace, mastering team dynamics is no longer a nice-to-have but a must-have skill for any organization to thrive.
{{inline-cta}}
In this article, we'll illustrate real life examples of both good and bad team dynamics in the workplace. Furthermore, we'll discuss some of the consequences that come from bad team dynamics, as well as tips on how you can improve your team dynamics.
Examples of good team dynamics in the workplace
The statistics are clear: high-performing teams get more done and have more fun while doing it. McKinsey’s studies have repeatedly shown the relationship between team performance and both team and individual output: top-performing leadership teams are three times likelier to generate above-average results, and individuals are five times more productive when working in a high-performing team than they are in an average one.
And it’s not just about getting work done. Members of high-performance teams also enjoy their work more. Psychologists studied 1,004 employees over five years and showed that high-performance contributes significantly to an individual’s satisfaction with their work. Group dynamics in the workplace can make all the difference.
So what constitutes a team with good team dynamics? Here are 8 things you can look for, with real life examples of how teams exhibit these effective team dynamics.
1. Clear communication
Clear communication is the backbone of any successful team. It's like a high-octane engine - when every gear understands its role, the whole machine runs smoothly. And it's not just about talking more; it's about making sure every team member understands the goals, tasks, and feedback. For example, let's say your team is building a rocket for a science project. If everyone knows exactly what part they're responsible for and when to do it, you're more likely to see that rocket soar high!
Want to benchmark your team's communication? Check out TeamVitals, our free team health score , and discover your team's level of transparency and alignment.
Let's imagine a marketing team working on a new campaign. Clear communication would involve the team members openly discussing their ideas, actively listening to each other, and providing feedback without hesitation. They would articulate their thoughts clearly and succinctly, ensuring everyone understands the objectives, timelines, and expectations. With clear communication, the team can collaborate effectively, leverage their diverse skills, and create a successful campaign.
As a leader, you can encourage clear communication by setting an example. Be open, honest, and clear with your expectations and feedback. And remember, it's a two-way street - listen to your team members and value their input. As a teammate, you can do your part by being open to feedback and willing to discuss issues. You can also ask questions if something isn't clear. Going back to our rocket example, it's like making sure everyone knows what their part looks like, where it goes, and asking if anyone needs help. By fostering this environment of openness and collaboration, you're helping your team's communication—and that rocket—soar to new heights!
2. Natural collaboration
When a team naturally collaborates, they're like a well-oiled machine. It's not just about working together, but working together effortlessly. Picture a basketball team. The players pass the ball to each other without even looking. They know where their teammates are, they trust them to be there, and they work together to score points. That's natural collaboration. It's not forced or awkward. It just flows.
You'll know natural collaboration when you see it. The signs? People freely sharing ideas, asking for input, and building on each other's thoughts. For example, in a brainstorming session, does one person's idea inspire another's? That's natural collaboration. It's a sign that people feel comfortable sharing and that they value each other's input.
To foster natural collaboration, start by creating an open, non-judgmental atmosphere where everyone feels comfortable sharing ideas. As a leader, encourage input and appreciate every idea. As a teammate, be open to other's ideas and be willing to build upon them. Remember, natural collaboration is like a muscle - the more you use it, the stronger it gets. So, keep exercising those collaboration muscles, and before you know it, your team will be passing the ball like pros.
Wondering whether you have a healthy, effective team? Looking for a great activity to use for team building? Download our free Team Health Scorecard and find out today.
3. Supportive and positive environment
A supportive environment is like a safety net for team members. It's knowing that when you take a risk or face a challenge, your team will be there to help you, not judge you. Imagine a new employee who's struggling with a task. Instead of ignoring her or criticizing her, her teammates step in to offer help and guidance. That's a supportive environment in action - it's about lifting each other up, not knocking each other down.
Spotting a supportive environment is often as simple as listening to how team members talk to each other. Are they patient and understanding? Do they offer help without being asked? For instance, if a member of a marketing team is having trouble with a presentation, do his colleagues offer to review his slides, give feedback, and share tips from their own experiences? That's a sign of a supportive environment.
Building a supportive environment starts with setting an example. As a leader, make sure to offer help and support to your team members, and recognize them when they do the same. As a teammate, be there for your colleagues, even when you're busy or stressed. It's not always easy, but the pay-off - a team that's more resilient, more cooperative, and more successful - is worth it.
4. Healthy competition
Healthy competition is a key driver for motivation and innovation in any team. It's like a friendly race, where everyone's trying to do their best while also cheering on their colleagues. Imagine a sales team where each member is striving to make the most sales. They're all aiming for the top spot, but they also share tips and cheer each other on. That's healthy competition - it pushes everyone to excel without creating a cutthroat environment.
Recognizing healthy competition isn't hard. Look for teams where everyone is motivated and energized, where they're all pushing to do their best but also celebrating each other's successes. For example, in a design team, one member might create an amazing new logo. Instead of feeling jealous, his teammates are inspired. They congratulate him and then get to work, each trying to come up with their own great design.
Encouraging healthy competition is a delicate balance. As a leader, it's important to set clear, fair rules for any competition and to ensure that everyone feels recognized for their contributions. As a teammate, it's important to engage in competition in a spirit of fairness and respect. Remember, the goal is not just to win, but to make everyone in the team better.
5. Constructive feedback
Constructive feedback is an essential building block of high-performing teams. It's the process of providing helpful, specific, and positive suggestions to improve performance and development. Think about a scenario where a graphic designer is working on a brand's logo. Her team leader doesn't just say, "I don't like it." Instead, he gives specific suggestions like, "Let's try using our company colors," or "Could you make the font a bit more modern?" This feedback is constructive, actionable, and encourages growth.
Spotting constructive feedback is as simple as observing communication that aims to build, not break. It is not personal, not generic, and not negative without a purpose. It's about growth and improvement. An example could be a software developer receiving feedback from a peer, "Your code works well, but it might be more efficient if you consider using this algorithm instead. It could reduce the execution time."
Encouraging the development of constructive feedback within a team is a shared responsibility. As a leader, foster an environment where feedback is seen as a tool for improvement, not as criticism. Regularly share constructive feedback and be open to receiving it. As a teammate, practice giving and receiving feedback respectfully and professionally. Remember, the goal of feedback is to help each other grow and make the team stronger.
6. Strong leadership
Leadership is a critical component of any successful team. However, strong leadership goes beyond just giving orders. It involves guiding the team towards its goals, empowering team members, and fostering a positive work environment. For example, a project manager at a tech company doesn't just assign tasks; she takes the time to understand her team members' strengths, delegates tasks accordingly, and provides constructive feedback to help them grow.
Recognizing strong leadership isn't always about grand gestures. It's often seen in the day-to-day operations of the team. Look for leaders who maintain open lines of communication, demonstrate empathy, and take responsibility when things go wrong. A sales team leader, for instance, doesn't blame his team when a deal falls through. Instead, he analyzes what went wrong, shares the learnings with the team, and strategizes on how to improve moving forward.
To cultivate strong leadership, it's essential to promote transparency, accountability, and continuous learning. As a leader, model these behaviors. For instance, be open about the team's progress, take responsibility for your actions, and show a willingness to learn and improve. As a teammate, support your leader in these endeavors. Offer feedback when necessary and step up to take the lead when you can. Remember, leadership is not just about leading others; it's about leading oneself as well.
7. Effective conflict resolution
When you picture a great team, you might imagine a group that never disagrees. But that's not the whole picture. Even the best teams face conflicts, and it's their ability to resolve these effectively that sets them apart. Effective conflict resolution means turning disagreements into opportunities for growth, rather than letting them breed resentment or stall progress. For instance, if two graphic designers disagree on a design element, rather than insisting on their own ideas, they brainstorm and come up with a better design that incorporates both their viewpoints.
Recognizing effective conflict resolution in a team can be quite simple. Look for disagreements that end in understanding, not standoffs. Check if conflicts lead to better solutions, not lingering resentment. For instance, in a project team, if there's a disagreement about the project timeline, does it devolve into a blame game, or does it lead to a productive discussion about how to manage time and resources more effectively?
As a leader, foster an environment where disagreement is allowed, but disrespect is not. Encourage open communication and active listening. When conflicts arise, guide your team to focus on the problem, not the person. As a teammate, approach disagreements with an open mind and a willingness to understand the other viewpoint. Remember, the goal is not to 'win' the argument, but to find the best solution for the team. This way, conflicts can become stepping stones to innovation, rather than roadblocks to success.
8. Collective ownership of team goals
Ever seen a football team celebrate a goal? That's collective ownership of team goals in action. In the workplace, it's about everyone feeling invested in the success of the team, not just their individual tasks. When a team shares this kind of mindset, their unity shows in their enthusiasm, shared problem-solving, and a sense of satisfaction when team goals are reached. For example, a marketing team might not only be excited about their individual tasks, like writing copy or designing ads, but also about the overall goal of boosting the company's brand recognition.
Recognizing collective ownership is like picking up on a team's vibe. Are team members just checking off their personal task lists, or are they actively engaged in the broader team goals? Do they celebrate team wins together, or only when they've personally succeeded? Let's consider a software development team: if a bug pops up, is everyone's first thought, "Not my code, not my problem," or do they come together to find a solution because they understand that the quality of the product is a shared responsibility?
Fostering collective ownership starts with clear, shared goals. As a leader, communicate the big picture and how each person's work contributes to it. Celebrate team achievements, not just individual ones. As a teammate, remind yourself that the team's success is your success. Offer help when you can and accept help when you need it. The beauty of collective ownership is that it's a team effort – much like scoring that goal in football. By encouraging this mindset, you can transform a group of individuals into a cohesive, high-performing team.
Examples of bad team dynamics in the workplace
However, there are just as many examples of bad team dynamics. And, while effective team dynamics lead to happier, higher-performing teams, ineffective team dynamics lead to the opposite outcomes: decreased productivity and morale, increased turnover and absenteeism, negative impact on team and individual performance, loss of trust and respect among team members, and even harmful effects on mental health and well-being. In fact, people sometimes point to examples of a bad team member that actually reflect examples of bad team dynamics!
Here are five things to look out for to suggest that teams are not exhibiting effective team dynamics.
1. Lack of communication and poor collaboration among team members
Just like a game of charades gone wrong, lack of communication in a team is easy to spot. Do you notice teammates often seem surprised or confused about tasks? Do team members feel out of the loop or find out about decisions too late? It's like showing up for a test you didn't know was scheduled. These are clear signs that communication within the team isn't up to par.
Imagine being part of a school project where each person has a part to play. Your task is to create a presentation, but you're not told the topic until the last minute. The result? A rushed, poor quality project that leaves everyone frustrated. This is what can happen in a team when there's a lack of communication.
As a leader, think of yourself as a football coach. It's your job to make sure everyone knows the game plan. Regular team meetings, clear instructions, and open-door policies can help. Also, promoting a culture where questions are encouraged can eliminate confusion.
If you're a teammate, don't hesitate to ask for clarification like you would in class. Proactively share updates about your work and encourage others to do the same. Remember, in a successful team, everyone is both a talker and a listener. Just like a successful band, everyone needs to know the song to play in harmony.
2. Formation of cliques or sub-groups
Workplace cliques can feel eerily similar to those high school lunchroom divides. If certain groups of coworkers always huddle up for coffee breaks, lunches, or office discussions, leaving others out, then you might have a clique situation. It's like being back at school, with a cool kids' table and everyone else scattered around.
Think of it this way: you're in a team of five working on a new product launch. Three of the members, who are close friends, make all the decisions among themselves. They conduct mini-meetings without including the rest of the team. As a result, the other two members often feel excluded and unheard, like they're on the outside looking in. This is how cliques can affect teamwork and productivity in an office setting.
If you're a leader, think of yourself as a fair and just king or queen. Promote a culture of inclusivity by ensuring everyone has a voice in decisions, rotate team tasks, and encourage collaboration among all team members. It's about making sure that everyone in the kingdom feels valued and included.
As a teammate, expand your circle. Talk to different people during breaks, ask for their input on projects, and share your own insights with them. It's like being the friendly student in class who chats with everyone. By doing this, you can help break down the walls of cliques and build a more cohesive and cooperative team.
3. Lack of trust
A lack of trust in a team can feel like trying to finish a group project, but no one wants to share their research. If you notice team members frequently double-checking each other's work, hesitating to share ideas, or not relying on their teammates for help, it's likely there's a trust issue. It's like everyone is playing a game of chess and doesn't want to reveal their moves.
Imagine a relay race where each runner is hesitant to pass the baton, fearing the next person might drop it. This slows down the entire team and reduces their chances of winning. Similarly, in a team project, if members don't trust each other's abilities or intentions, it can slow progress and create an uncomfortable environment.
As a leader, think of yourself as the team's coach. You can foster trust by assigning tasks that allow team members to showcase their skills, encouraging open communication, and praising team achievements. It's like creating a safe playground where everyone feels confident to try new things.
If you're a team member, be reliable, like the friend who always shows up when they promise to. Deliver your work on time, be open to feedback, and offer your help to others. By demonstrating your trustworthiness, you can help build a stronger bond of trust within the team. Remember, every successful team, like a well-rehearsed band, is built on trust.
4. Overdependence on one person
Overdependence on one person in a team can feel like being in a kitchen where only the head chef is doing all the cooking, prepping, and cleaning. If you observe one team member constantly overloaded with tasks while others are idle, or decisions always hinge on one person's input, then it's likely the team is leaning too heavily on one individual. It's akin to a music band where only one member is expected to sing, play instruments, and write songs.
Consider a software development team where one programmer is the only person who understands a critical part of the code. They're always on call, fixing bugs, and adding new features, while the rest of the team is underutilized. This over-reliance can lead to burnout for that individual, and risk for the project if that person is ever unavailable.
As a leader, see yourself as the conductor of an orchestra. Your role is to ensure every musician plays their part. Distribute tasks evenly, encourage team members to develop a variety of skills, and foster a culture where everyone's input is valued. It's about making sure everyone gets a chance to contribute to the symphony.
As a teammate, don't hesitate to step in. If you notice someone drowning in tasks, offer to share the workload or use this as an opportunity to learn and expand your own skills. By doing this, you help create a more balanced team that can hit all the right notes. Remember, a team, like a successful orchestra, functions best when everyone plays their part.
5. No clear goals
A team without clear goals can feel like a ship sailing without a map. If you find your team members often confused about their tasks, unsure of what the team's priorities are, or if projects seem to drift without a clear endpoint, then there's likely a lack of clear goals. It's similar to a band trying to play a song without knowing the tune.
Imagine a marketing team launching a new campaign. Without clear goals, one team member focuses on increasing social media followers, another is dedicated to website traffic, and another is trying to boost newsletter subscriptions. They're all working hard, but not in a coordinated way. It's like everyone rowing a boat in different directions.
As a leader, you're like the captain of a ship. You need to set the course and make sure everyone on board knows the destination. Clearly define the team's goals, ensure everyone understands their role in reaching those goals, and regularly check-in to keep everyone on track.
As a teammate, don't be afraid to ask for clarity. If you're unsure about the team's goals or your role in achieving them, seek clarification. Also, share your progress regularly and align your work with the team's goals. It's like tuning your instrument to match the rest of the band. With clear goals, everyone can play in harmony.
6. Conflict avoidance
Conflict avoidance in a team can be like a group of friends who never disagree - not because they always think alike, but because they're afraid to argue. If team members often agree quickly without much discussion, or if problems persist without being addressed, then the team might be avoiding conflict. It's like a band whose members never discuss which song to play next, leading to a repetitive playlist.
Consider a product design team. One member consistently misses deadlines, causing delays. Instead of addressing this, the team adjusts their own schedules to compensate. This is like a band adjusting their tempo to a drummer who can't keep time, instead of helping them improve.
As a leader, think of yourself as a referee in a sports game. Your job is to ensure fair play, not to prevent all conflicts. Encourage open and respectful discussions, create a safe environment for feedback, and guide your team in addressing conflicts productively.
As a teammate, don't shy away from disagreement. Remember, it's like suggesting a new song to your band - it might lead to a discussion, but it can also lead to a better playlist. Express your opinions respectfully, listen to others, and work together to find solutions. With the right approach, conflict can be a tool for improvement, not a problem to avoid.
7. Too much competition
Too much competition in a team can be like a sports team where every player is trying to score themselves, instead of working together to win the game. If team members seem more focused on outdoing each other than on achieving the team's goals, or if they're reluctant to share information and resources, you're probably dealing with excessive competition. It's akin to a band where everyone tries to play a solo at the same time, leading to a chaotic performance.
Imagine a sales team where every member is so focused on being the top seller that they withhold successful strategies from each other and even sabotage their teammates' efforts. The result is a hostile environment that hinders the overall sales performance. It's like a soccer team where everyone wants to be the star player, but they end up losing the match.
As a leader, think of yourself as the band's conductor. You should encourage harmony, not discord. Foster a culture of collaboration over competition by setting team-based goals and rewards, promoting knowledge sharing, and celebrating collective achievements.
As a teammate, remember, it's not about outshining everyone else, but about contributing to the team's success. Be open to sharing resources and ideas, and support your colleagues' efforts. It's like playing your part in the band to create a beautiful symphony, not a cacophony. When competition is balanced with cooperation, everyone wins.
8. Micromanagement
Micromanagement in a team can feel like a teacher constantly looking over your shoulder as you take a test. If a team leader is always checking every detail of work, or if team members aren't given the freedom to make decisions or take initiative, then micromanagement could be the problem. It's like a band leader telling each musician not just what to play, but exactly how to play it.
Consider a graphic design team where the manager insists on approving every color, font, and layout choice. The designers feel their creativity is stifled and their time wasted on endless revisions. It's like a conductor telling a violinist which fingers to use for every note, instead of trusting their expertise.
As a leader, remember, you're a guide, not a puppet master. Set clear expectations, then trust your team to meet them. Provide guidance and feedback, but avoid dictating every step. It's like giving the band the sheet music and letting them bring it to life.
As a teammate, communicate your concerns diplomatically and demonstrate your competence. Show that you can hit the right notes without someone constantly adjusting your strings. When leaders and teammates trust each other to do their part, the whole team performs in harmony.
Tips for improving team dynamics
1. begin with a benchmark for how your team works.
To benchmark how a team works, a team leader should first define the team's goals and objectives. They should then identify key performance indicators (KPIs) to measure progress towards those goals. Next, they can analyze the team's current performance against those KPIs and identify areas for improvement.
Consider a team personality test like TeamDynamics to quantitatively define how your team communicates and collaborates to get work done.
The team leader should also gather feedback from team members to understand their perspectives and identify opportunities to enhance collaboration and communication. Finally, the team leader should regularly review and adjust the benchmarking approach to ensure continuous improvement and alignment with the team's evolving needs.
2. Prioritize communication and collaboration
A team leader should prioritize communication and collaboration by setting clear expectations and promoting open dialogue among team members. This can be achieved by establishing regular check-ins and encouraging feedback from team members. Additionally, the leader should create a culture of transparency and inclusivity, where all members feel valued and heard. It's also important for the leader to model good communication and collaboration practices and to provide training and resources to team members as needed. By prioritizing communication and collaboration, a team leader can build a strong, cohesive team that is able to achieve its goals effectively.
3. Create a supportive and positive work environment
To create a supportive and positive work environment, a team leader should start by fostering open and honest communication. They should encourage their team members to share their thoughts and ideas, and provide them with the resources they need to succeed. Additionally, a team leader should actively promote teamwork and collaboration, and recognize and reward their team members' achievements. They should also be approachable and empathetic, and be willing to provide support and guidance when needed. Finally, a team leader should lead by example and demonstrate a positive attitude, as their behavior can set the tone for the entire team.
4. Foster healthy competition and constructive feedback
To foster healthy competition and constructive feedback in a team, a leader should first establish clear performance metrics and goals that are attainable yet challenging. Encourage team members to support and collaborate with each other while still maintaining a level of healthy competition. Provide regular constructive feedback to each team member and encourage them to provide feedback to each other in a constructive manner. Celebrate team successes and encourage members to learn from any failures or setbacks. Encourage a culture of continuous improvement and provide opportunities for skill-building and professional development.
5. Encourage collective ownership of team goals and responsibilities
A team leader can encourage collective ownership of team goals and responsibilities in several ways. Firstly, they should ensure that every team member understands their role and how their contributions fit into the bigger picture. Secondly, they can create opportunities for collaboration and teamwork, such as group brainstorming sessions or team-building activities. Thirdly, they should provide regular feedback and recognition to individual team members for their contributions. Fourthly, they can facilitate regular team meetings to discuss progress, challenges, and solutions. Finally, the team leader should lead by example and show their commitment to the team's goals by actively participating and modeling the desired behaviors.
The bottom line is that high-performing teams don’t just happen. They are the result of understanding your team dynamics and using that understanding to create the right environment for success. Applied properly, team dynamics provide a robust vocabulary and toolkit to enhance your team’s effectiveness. And when a team gets it right, the results can be spectacular.
Enjoyed this read?
Get updates whenever we post more content like this. Unsubscribe anytime.
When we have team meetings…
Our team understands what it's being asked to do., how well do you know your team.
We've analyzed thousands of teams across industries, functions, and geographies. Here's a few things we've found.
Understanding how your team works is the key to getting work done (and having fun while doing it). You might be surprised what you learn.
TeamDynamics is a tool for individuals and teams who believe that teamwork should be intentional and rewarding.
We spend just as much time today with our coworkers as we do with our loved ones. We have tools to manage our relationships with partners: love languages, compatibility tests, therapy, and more.
But when it comes to relationships with our professional teams, we're flying blind. It doesn't have to be that way.
TeamDynamics is a team building tool to help the modern team get more done and have more fun while doing it. Quantify your team's behaviors. Describe them with a shared language. Improve your team's performance with tailored recommendations.

"I've used TeamDynamics with a range of clients. Each time, it's helped me quickly understand the team I'm working with, leading to faster results and happier clients. A must-have for consultants!"

"When I switched teams, I felt like I lost my instincts for working with my colleagues: things that were easy to coordinate before seemed to take forever, and I couldn't get my points across. TeamDynamics helped me get my groove back."

"I've managed teams for two decades. Haven't seen many personality tests that can rival TeamDynamics for practicality. Notably enhanced our team's cohesion and productivity."
Discover your team's personality.
Learn how your team works. Unlock your team's potential. Get your TeamDynamics today.
More like this:

7 Behaviors That Build Trust in Virtual Teams and Hybrid Teams

How to Use ChatGPT to Give Employee Feedback

How to Use ChatGPT to Plan Your Next Team Offsite
Do you know your team's personality 🤔.
TeamDynamics describes how your team works together and how you fit in. We'll send you a sample so you can check it out for yourself!
- 1-800-565-8735
- [email protected]
16 Team Building Case Studies and Training Case Studies
From corporate groups to remote employees and everything in between, the key to a strong business is creating a close-knit team. in this comprehensive case study, we look at how real-world organizations benefited from team building, training, and coaching programs tailored to their exact needs. .
Updated: December 21, 2021
We’re big believers in the benefits of team building , training and development , and coaching and consulting programs. That’s why our passion for helping teams achieve their goals is at the core of everything we do.
At Outback Team Building & Training, our brand promis e is to be recommended , flexible, and fast. Because we understand that when it comes to building a stronger and more close-knit team, there’s no one-size-fits-all formula. Each of our customers have a unique set of challenges, goals, and definitions of success.
And they look to us to support them in three key ways: making their lives easy by taking on the complexities of organizing a team building or training event; acting fast so that they can get their event planned and refocus on all the other tasks they have on their plates, and giving them the confidence that they’ll get an event their team will benefit from – and enjoy.
In this definitive team building case study , we’ll do a deep dive into real-world solutions we provided for our customers.
4 Unique Team Building Events & Training Programs Custom-Tailored for Customer Needs
1. a custom charity event for the bill & melinda gates foundation , 2. how principia built a stronger company culture even with its remote employees working hundreds of miles apart , 3. custom change management program for the royal canadian mint, 4. greenfield global uses express team building to boost morale and camaraderie during a challenging project, 5 virtual team building activities to help remote teams reconnect, 1. how myzone used virtual team building to boost employee morale during covid-19, 2. americorps equips 90 temporary staff members for success with midyear virtual group training sessions, 3. how microsoft’s azure team used virtual team building to lift spirits during the covid-19 pandemic, 4. helping the indiana cpa society host a virtual team building activity that even the most “zoom fatigued” guests would love, 5. stemcell brightens up the holiday season for its cross-departmental team with a virtually-hosted team building activity, 3 momentum-driving events for legacy customers, 1. how a satellite employee “garnered the reputation” as her team’s pro event planner, 2. why plentyoffish continues to choose ‘the amazing race’ for their company retreat, 3. how team building helped microsoft employees donate a truckload of food, 4 successful activities executed on extremely tight timelines, 1. finding a last-minute activity over a holiday, 2. from inquiry to custom call in under 30 minutes, 3. a perfect group activity organized in one business day, 4. delivering team building for charity in under one week.

We know that every team has different needs and goals which is why we are adept at being flexible and have mastered the craft of creating custom events for any specifications.

When the Seattle, Washington -based head office of the Bill & Melinda Gates Foundation – a world-renowned philanthropic organization – approached us in search of a unique charity event, we knew we needed to deliver something epic. Understanding that their team had effectively done it all when it comes to charity events, it was important for them to be able to get together as a team and give back in new ways .
Our team decided the best way to do this was to create a brand-new event for the Bill & Melinda Gates Foundation which had never been executed before. We created an entirely new charitable event – Bookworm Builders – for them and their team loved it! It allowed them to give back to their community, collaborate, get creative, and work together for a common goal. Bookworm Builders has since gone on to become a staple activity for tons of other Outback Team Building & Training customers!
To learn more about how it all came together, read the case study: A Custom Charity Event for the Bill & Melinda Gates Foundation .

Who said hosting an impactful training program means having your full team in the same place at the same time? Principia refused to let distance prevent them from having a great team, so they contacted us to help them find a solution. Their goals were to find better ways of working together and to create a closer-knit company culture among their 20 employees and contractors living in various parts of the country.
We worked with Principia to host an Emotional Intelligence skill development training event customized to work perfectly for their remote team. The result was a massive positive impact for the company. They found they experienced improved employee alignment with a focus on company culture, as well as more emotionally aware and positive day-to-day interactions. In fact, the team made a 100% unanimous decision to bring back Outback for additional training sessions.
To learn more about this unique situation, read the full case study: How Principia Built a Stronger Company Culture Even with its Remote Employees Working Hundreds of Miles Apart .
We know that employee training that is tailored to your organization can make the difference between an effective program and a waste of company time. That’s why our team jumped at the opportunity to facilitate a series of custom development sessions to help the Royal Canadian Mint discover the tools they needed to manage a large change within their organization.
We hosted three custom sessions to help the organization recognize the changes that needed to be made, gain the necessary skills to effectively manage the change, and define a strategy to implement the change:
- Session One: The first session was held in November and focused on preparing over 65 employees for change within the company.
- Session Two: In December, the Mint’s leadership team participated in a program that provided the skills and mindset required to lead employees through change.
- Session Three: The final session in February provided another group of 65 employees with guidance on how to implement the change.
To learn more, read the full case study: Custom Change Management Program for the Royal Canadian Mint .

When Greenfield Global gathered a team of its A-Players to undertake a massive, challenging project, they knew it was important to build rapports among colleagues, encourage collaboration, and have some fun together.
So, we helped them host an Express Clue Murder Mystery event where their team used their unique individual strengths and problem-solving approaches in order to collaboratively solve challenges.
To learn more, read the full case study: Greenfield Global Uses Express Team Building to Boost Morale and Camaraderie During a Challenging Project .

When the COVID-19 pandemic struck, we were proud to be able to continue supporting our customers’ goals with virtual team building activities and group training sessions.

With remote work being mandated as self-quarantine requirements are enforced on a global scale, companies began seeking ways to keep their newly-remote teams engaged and ensure morale remained as high as possible.
And MyZone was no exception. When the company found themselves feeling the effects of low employee morale and engagement, they noticed a decrease in productivity and motivation.
To make matters even more difficult, MyZone’s team works remotely with employees all over the world. This physical distancing makes it challenging for them to build a strong rapport, reinforce team dynamics, and boost morale and engagement.
The company was actively searching for an activity to help bring their employees closer together during this challenging time but kept running into a consistent issue: the majority of the team building activities they could find were meant to be done in person.
They reached out to Outback Team Building and Training and we were able to help them achieve their goals with a Virtual Clue Murder Mystery team building activity.

AmeriCorps members are dedicated to relieving the suffering of those who have been impacted by natural disasters. And to do so, they rely on the support of a team of temporary staff members who work one-year terms with the organization. These staff focus on disseminating emergency preparedness information and even providing immediate assistance to victims of a disaster.
During its annual midyear training period, AmeriCorps gathers its entire team of temporary staff for a week of professional development seminars aimed at both helping them during their term with the company as well as equipping them with skills they can use when they leave AmeriCorps.
But when the COVID-19 pandemic got underway, AmeriCorps was forced to quickly re-evaluate the feasibility of its midyear training sessions.
That’s when they reached out to Outback. Rather than having to cancel their midyear training entirely, we were able to help them achieve their desired results with four virtual group training sessions: Clear Communication , Performance Management Fundamentals , Emotional Intelligence , and Practical Time Management .
Find all the details in the full case study: AmeriCorps Equips 90 Temporary Staff Members for Success with Midyear Virtual Training Sessions.

With the COVID-19 pandemic taking a significant toll on the morale of its employees, Microsoft’s Azure team knew they were overdue for an uplifting event.
It was critical for their team building event to help staff reconnect and reengage with one another. But since the team was working remotely, the activity needed to be hosted virtually and still be fun, engaging, and light-hearted.
When they reached out to Outback Team Building and Training, we discussed the team’s goals and quickly identified a Virtual Clue Murder Mystery as the perfect activity to help their team get together online and have some fun together.
For more information, check out the entire case study: How Microsoft’s Azure Team Used Virtual Team Building to Lift Spirits During the COVID-19 Pandemic.

The Indiana CPA Society is the go-to resource for the state’s certified public accountants. The organization supports CPAs with everything from continuing education to networking events and even advocacy or potential legislation issues that could affect them.
But as the time approached for one of INCPAS’ annual Thanksgiving event, the Indiana CPA Society’s Social Committee needed to plan a modified, pandemic-friendly event for a group of people who were burnt out my online meetings and experiencing Zoom fatigue.
So, we helped the team with a Self-Hosted Virtual Code Break team building activity that INCPAS staff loved so much, the organization decided to host a second event for its Young Pros and volunteers.
For INCPAS’ Social Committee, the pressure to put on an event that everyone will enjoy is something that’s always on their mind when planning out activities. And their event lived up to their hopes.
For more information, check out the entire case study: Helping the Indiana CPA Society Host a Virtual Team Building Activity That Even the Most “Zoom Fatigued” Guests Would Love .

When Stemcell was looking for a way to celebrate the holidays, lift its team members’ spirits, and help connect cross-departmental teams during the pandemic, they contacted us to help host the perfect team building activity.
They tasked us with finding an event that would help team members connect, get in the holiday spirit, and learn more about the business from one another during the midst of a stressful and challenging time.
So, we helped them host a festive, virtually-hosted Holiday Hijinks team building activity for employees from across the company.
For more information, check out the entire case study: Stemcell Brightens Up the Holiday Season for its Cross-Departmental Team with a Virtually-Hosted Team Building Activity .

We take pride in being recommended by more than 14,000 corporate groups because it means that we’ve earned their trust through delivering impactful results.
We’ve been in this business for a long time, and we know that not everybody who’s planning a corporate event is a professional event planner. But no matter if it’s their first time planning an event or their tenth, we love to help make our customers look good in front of their team. And when an employee at Satellite Healthcare was tasked with planning a team building event for 15 of her colleagues, she reached out to us – and we set out to do just that!
Our customer needed a collaborative activity that would help a diverse group of participants get to know each other, take her little to no time to plan, and would resonate with the entire group.
With that in mind, we helped her facilitate a Military Support Mission . The event was a huge success and her colleagues loved it. In fact, she has now garnered a reputation as the team member who knows how to put together an awesome team building event.
To learn more, read the case study here: How a Satellite Employee “Garnered the Reputation” as Her Team’s Pro Event Planner .

In 2013, international dating service POF (formerly known as PlentyOfFish) reached out to us in search of an exciting outdoor team building activity that they could easily put to work at their annual retreat in Whistler, B.C . An innovative and creative company, they were in search of an activity that could help their 60 staff get to know each other better. They also wanted the event to be hosted so that they could sit back and enjoy the fun.
The solution? We helped them host their first-ever Amazing Race team building event.
Our event was so successful that POF has now hosted The Amazing Race at their annual retreat for five consecutive years .
To learn more, check out our full case study: Why PlentyOfFish Continues to Choose ‘The Amazing Race’ for Their Company Retreat .

As one of our longest-standing and most frequent collaborators, we know that Microsoft is always in search of new and innovative ways to bring their teams closer together. With a well-known reputation for being avid advocates of corporate social responsibility, Microsoft challenged us with putting together a charitable team building activity that would help their team bond outside the office and would be equal parts fun, interactive, and philanthropic.
We analyzed which of our six charitable team building activities would be the best fit for their needs, and we landed on the perfect one: End-Hunger Games. In this event, the Microsoft team broke out into small groups, tackled challenges like relay races and target practice, and earned points in the form of non-perishable food items. Then, they used their cans and boxes of food to try and build the most impressive structure possible in a final, collaborative contest. As a result, they were able to donate a truckload of goods to the local food bank.
For more details, check out the comprehensive case study: How Team Building Helped Microsoft Employees Donate a Truckload of Food .
Time isn’t always a luxury that’s available to our customers when it comes to planning a great team activity which is why we make sure we are fast, agile, and can accommodate any timeline.

Nothing dampens your enjoyment of a holiday more than having to worry about work – even if it’s something fun like a team building event. But for one T-Mobile employee, this was shaping up to be the case. That’s because, on the day before the holiday weekend, she found out that she needed to organize a last-minute activity for the day after July Fourth.
So, she reached out to Outback Team Building & Training to see if there was anything we could do to help – in less than three business days. We were happy to be able to help offer her some peace of mind over her holiday weekend by recommending a quick and easy solution: a Code Break team building activity. It was ready to go in less than three days, the activity organized was stress-free during her Fourth of July weekend, and, most importantly, all employees had a great experience.
For more details, check out the full story here: Finding a Last-Minute Activity Over a Holiday .

At Outback Team Building & Training, we know our customers don’t always have time on their side when it comes to planning and executing an event. Sometimes, they need answers right away so they can get to work on creating an unforgettable experience for their colleagues.
This was exactly the case when Black & McDonald approached us about a learning and development session that would meet the needs of their unique group, and not take too much time to plan. At 10:20 a.m., the organization reached out with an online inquiry. By 10:50 a.m., they had been connected with one of our training facilitators for a more in-depth conversation regarding their objectives.
Three weeks later, a group of 14 Toronto, Ontario -based Black & McDonald employees took part in a half-day tailor-made training program that was built around the objectives of the group, including topics such as emotional intelligence and influence, communication styles, and the value of vulnerability in a leader.
To learn more about how this event was able to come together so quickly, check out the full story: From Inquiry to Custom Call in Under 30 Minutes .

When Conexus Credit Union contacted us on a Friday afternoon asking if we could facilitate a team building event for six employees the following Monday morning, we said, “Absolutely!”
The team at Conexus Credit Union were looking for an activity that would get the group’s mind going and promote collaboration between colleagues. And we knew just what to recommend: Code Break Express – an activity filled with brainteasers, puzzles, and riddles designed to test the group’s mental strength.
The Express version of Code Break was ideal for Conexus Credit Union’s shorter time frame because our Express activities have fewer challenges and can be completed in an hour or less. They’re self-hosted, so the company’s group organizer was able to easily and efficiently run the activity on their own.
To learn more about how we were able to come together and make this awesome event happen, take a look at our case study: A Perfect Group Activity Organized in One Business Day .

We’ve been lucky enough to work with Accenture – a company which has appeared on FORTUNE’s list of “World’s Most Admired Companies” for 14 years in a row – on a number of team building activities in the past.
The organization approached us with a request to facilitate a philanthropic team building activity for 15 employees. The hitch? They needed the event to be planned, organized, and executed within one week.
Staying true to our brand promise of being fast to act on behalf of our customers, our team got to work planning Accenture’s event. We immediately put to work the experience of our Employee Engagement Consultants, the flexibility of our solutions, and the organization of our event coordinators. And six days later, Accenture’s group was hard at work on a Charity Bike Buildathon , building bikes for kids in need.
To learn more about how we helped Accenture do some good in a short amount of time, read the full case study: Delivering Team Building for Charity in Under One Week .
Learn More About Team Building, Training and Development, and Coaching and Consulting Solutions
For more information about how Outback Team Building & Training can help you host unforgettable team activities to meet your specific goals and needs on virtually any time frame and budget, just reach out to our Employee Engagement Consultants.
Subscribe To Our Newsletter
And stay updated, related articles.

The 5 Best Remote Teamwork Tactics to Implement in 2024

How to Create an Engaging And Productive Virtual Internship Program

How to Develop an Employee Volunteer Training Program

From corporate groups to remote employees and everything in between, the key to a strong business is creating a close-knit team. That’s why you need to do team-building sessions as much as you can.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
Barriers and enablers to effective interprofessional teamwork in the operating room: A qualitative study using the Theoretical Domains Framework
Cole etherington.
1 Department of Anaesthesiology and Pain Medicine, University of Ottawa, Ottawa, Ontario, Canada
2 Clinical Epidemiology Program, The Ottawa Hospital Research Institute, Ottawa, Ontario, Canada
Joseph K. Burns
Simon kitto.
3 Department of Innovation in Medical Education, University of Ottawa, Ottawa, Ontario, Canada
Jamie C. Brehaut
4 School of Epidemiology & Public Health, University of Ottawa, Ottawa, Ontario, Canada
Meghan Britton
5 Main Operating Room, The Ottawa Hospital, Ottawa, Ontario, Canada
Sukhbir Singh
6 Department of Obstetrics & Gynecology, University of Ottawa, Ottawa, Ontario, Canada
Sylvain Boet
7 Francophone Affairs, Faculty of Medicine, University of Ottawa, Ottawa, Ontario, Canada
8 Institut du Savoir Montfort, Ottawa, Ontario, Canada
9 Faculty of Education, University of Ottawa, Ottawa, Ontario, Canada
Associated Data
All relevant data are within the manuscript and its Supporting information files.
Effective teamwork is critical for safe, high-quality care in the operating room (OR); however, teamwork interventions have not consistently resulted in the expected gains for patient safety or surgical culture. In order to optimize OR teamwork in a targeted and evidence-based manner, it is first necessary to conduct a comprehensive, theory-informed assessment of barriers and enablers from an interprofessional perspective.
This qualitative study was informed by the Theoretical Domains Framework (TDF). Volunteer, purposive and snowball sampling were conducted primarily across four sites in Ontario, Canada and continued until saturation was reached. Interviews were recorded, transcribed, and de-identified. Directed content analysis was conducted in duplicate using the TDF as the initial coding framework. Codes were then refined whereby similar codes were grouped into larger categories of meaning within each TDF domain, resulting in a list of domain-specific barriers and enablers.
A total of 66 OR healthcare professionals participated in the study (19 Registered Nurses, two Registered Practical Nurses, 17 anaesthesiologists, 26 surgeons, two perfusionists). The most frequently identified teamwork enablers included people management, shared definition of teamwork, communication strategies, positive emotions, familiarity with team members, and alignment of teamwork with professional role. The most frequently identified teamwork barriers included others’ personalities, gender, hierarchies, resource issues, lack of knowledge of best practices for teamwork, negative emotions, conflicting norms and perceptions across professions, being unfamiliar with team members, and on-call/night shifts.
Conclusions
We identified key factors influencing OR teamwork from an interprofessional perspective using a theoretically informed and systematic approach. Our findings reveal important targets for future interventions and may ultimately increase their effectiveness. Specifically, achieving optimal teamwork in the OR may require a multi-level intervention that addresses individual, team and systems-level factors with particular attention to complex social and professional hierarchies.
Introduction
Effective teamwork is essential for safe, high-quality healthcare [ 1 , 2 ]. It is particularly important in the operating room (OR), where professionals of different disciplines, educational backgrounds, and experiences must work interdependently in a dynamic, high-stakes environment [ 3 – 10 ]. Studies have documented that OR teamwork “failures” (i.e. suboptimal practice) are very common: some indicate that teamwork issues happen to various degrees in every surgery [ 6 , 11 , 12 ] while others observe the rate of suboptimal teamwork practices to be as high as 17.4 per hour [ 13 ]. The odds of surgical complications are approximately five times higher when interprofessional teamwork is ineffective [ 6 ].
Although many studies have explored various facets of OR teamwork [ 14 – 16 ], there has yet to be a systematic assessment of teamwork barriers and enablers that can directly inform behavior change interventions. Instead, there has remained a gap between observational studies of teamwork offering in-depth accounts of practices within a particular context and interventional studies that aim to improve teamwork. For example, most interventions involve team training to improve some element of teamwork (e.g. communication) [ 17 ], yet observational research indicates that teamwork is a complex phenomenon influenced by multiple factors across multiple levels (i.e. individual, team, organization) [ 14 , 18 ]. A single-faceted strategy such as team training is unlikely to address the multilevel factors required for a substantial and sustainable improvement in OR teamwork as a whole. Not surprisingly, most teamwork interventions result in a limited effect on teamwork and associated outcomes [ 17 ]. In addition, there has not been any substantial reduction in patient safety events in recent years [ 19 , 20 ].
The Theoretical Domains Framework (TDF) is a tool used in the field of implementation science to close the gap between research and practice. It was specifically developed to elicit determinants of clinical behaviour and to inform the design of behaviour change interventions [ 21 , 22 ]. As a comprehensive framework comprised of key psychological theories and constructs, the TDF has been applied in a variety of healthcare settings to understand the factors driving current practice in order to change clinician behaviour [ 23 – 30 ]. Applying the TDF to behaviour (e.g. teamwork) allows its determinants (i.e. barriers and enablers) to be mapped to specific behaviour change techniques and modes of delivery [ 31 , 32 ]. This approach increases the likelihood of influencing healthcare professional behaviour in a meaningful and clinically significant way [ 23 , 32 , 33 ]. This study therefore aimed to identify factors that facilitate or impede OR teamwork from an interprofessional perspective using the TDF in order to inform future evidence-based, actionable interventions.
This study is reported in accordance with the Standards for Reporting Qualitative Research checklist [ 34 ]. Ethical approval was obtained from the Ottawa Health Science Network Research Ethics Board (#20170875; coordinating site) and the Unity Health Toronto Research Ethics Board (REB #18–396).
Study design
We conducted a prospective, multicentre qualitative study using semi-structured interviews, either in person or over the telephone, with OR healthcare providers. Participant informed consent was obtained from each participant by the study interviewers (JB, NE). For interviews conducted in person, the interviewer obtained informed written consent. For interviews conducted over the telephone, verbal consent was documented by the interviewer on the participant master list.
Setting and context
Recruitment primarily took place across six sites: one academic hospital located in Toronto, Canada and three academic hospitals located in Ottawa, Canada, one of which had three campuses. Each hospital performs a large volume of a wide range of surgical procedures, such as general, gynecological, trauma, pediatric, and cardiac surgeries, and both oncological and non-oncological surgeries. Participants at each site were invited to refer colleagues to the study as well, creating the possibility for representation of additional sites.
Sample and recruitment
All healthcare professionals working in the OR were eligible to participate, including scrub and circulating nurses, anaesthesiologists, perfusionists, anaesthesia assistants, surgeons, and anaesthesia and surgical post-graduate trainees. Across the six primary recruitment sites, there were over 1000 eligible healthcare professionals. Healthcare professionals not part of the OR team at these or referred sites were not eligible to participate. We used volunteer, purposive, and snowball sampling to optimize recruitment [ 35 ]. An invitation to participate in the study was emailed to the perioperative departments of each participating hospital site. Individuals participated in the study on a “first come, first served” basis, unless data saturation had occurred within their particular professional group. Participants were also invited to refer their colleagues from outside their centres to the study. Purposive sampling was used to obtain representativeness among professional groups where it was observed necessary (e.g. to obtain both male and female nurses). Participants were offered a gift card for participation upon completing their interview. Representativeness of the sample is limited, however, to OR team members at academic hospitals in Ontario, Canada, as this is where our primary recruitment took place.
Theoretical framework
A modified version of the Theoretical Domains Framework (TDF) [ 23 , 36 ], guided interview guide development, data collection, and analysis. The TDF is a validated framework for ascertaining barriers and facilitators to behaviour change among healthcare professionals [ 23 ]. It consists of 14 theoretical domains ( S1 Appendix ) derived from 128 theoretical constructs from 33 theories of behaviour and behaviour change relevant to determinants of behaviour and intervention development in healthcare [ 23 , 36 ]. The domains were derived through a systematic expert consensus process and provide a basis for understanding the broad set of factors that may influence behaviour. Although the TDF has been used to examine barriers and enablers to various behaviours across many healthcare settings [ 23 ], it has yet to be used to study interprofessional teams in the OR.
Interview guide
The semi-structured interview guide ( S2 Appendix ) developed by the co-investigator team comprised of practicing OR clinicians from anaesthesia, nursing, and surgery as well as researchers with backgrounds in medical education, qualitative research, implementation science, psychology, and sociology. The interdisciplinary background of the team helped to ensure the interview guide was comprehensive through inclusion of anaesthesia, nursing, and surgical perspectives as well as educational, sociological, and psychological considerations.
The guide included open-ended questions based on the TDF domains along with additional questions to explore aspects of social identity (e.g. gender, age, ethnicity) and teamwork for a separate study. The questions covered experiences and perspectives of teamwork according to participants’ professional contexts and explored factors influencing teamwork at the individual and team level. We pilot tested the interview guide with two OR clinicians (one physician and one nurse) to provide feedback on clarity of questions and revised the wording of several questions accordingly. The guide was iteratively revised throughout the interview process to better capture new themes introduced by participants and to remove or rephrase questions participants had difficulty answering, as per best practices in qualitative research [ 37 ]. Examples of questions asked include “How would you define teamwork?” ( knowledge ); “As a [profession], is there anything that influences your approach to teamwork in the OR?” ( social/professional role and identity ); “Do your emotions every influence whether or not you engage in good teamwork in the OR?” ( emotions ); and “Would any other team member influence whether or not you engage in good teamwork in the OR?” ( social influences ).
Interviewer training
Interviews were conducted in English by two research team members (JKB, NE) with no previous relationships to participants. The research team members were each trained in qualitative research methods and experienced in working within sensitive healthcare environments. Prior to conducting the interviews, the research team members familiarized themselves with the interview guide and conducted a practice interview. The interview guide was then further refined to facilitate conversation flow by adding several broad introductory questions (e.g. “What does teamwork mean to you?”) and re-ordering some of the other questions.
Data collection
Interviews were scheduled with interested participants over a four-month period (January to April 2019). Demographic information was collected from all participants (e.g. profession, years of experience, age, sex) at the time of their interview. Interviews continued until data saturation was reached, which was defined as conducting three interviews within each major professional group (anaesthesia, nursing, surgery) without the emergence of any new themes (after a minimum of 10 interviews per group) [ 38 ]. The interviewers met regularly to discuss themes emerging from the interviews and assess whether data saturation had been met.
Data analysis
Interviews were audio-recorded, transcribed, and de-identified. De-identified transcripts were imported into NVivo 12 (QSR International, Doncaster, Australia) for analysis. Deductive directed content analysis was conducted by two research team members (JKB, NE) using the TDF as the coding framework. To establish consistency between coders, three interviews were first coded independently; after which the two coders met to review their coding, resolve discrepancies, and determine a coding strategy. All remaining interview transcripts were then divided equally between the two coders and coded using the agreed upon coding scheme. The coders met frequently to triangulate the data and maintain reliability, with 10% of the remaining interviews coded in duplicate.
After data were coded into the TDF domains, data units (i.e. several lines of text) were labelled with codes according to the key concept represented within the data unit by one coder (NE). These codes were refined whereby similar codes were grouped into larger themes within each TDF domain. Findings were summarized within and across each main professional group (i.e. nursing, anaesthesia, surgery) and verified by a second coder (JKB). TDF domains were classified as relevant to intraoperative teamwork (i.e., more likely to influence teamwork) based on: the frequency of specific beliefs across interviews (four or more clinicians identified the belief in their interview), the number of beliefs in each domain (more than two), the presence of conflicting beliefs signaling variation in beliefs and attitudes, and evidence of strong beliefs that could directly influence teamwork performance [ 23 ]. Based on all these factors, we concurrently established domain relevance.
Participant characteristics
A total of 66 healthcare professionals who currently practice in the OR were interviewed ( Table 1 ). Of these, 19 (29.9%) were Registered Nurses (15 female, 4 male), two (3%) were Registered Practical Nurses (1 female, 1 male), 17 (25.8%) were anaesthesiologists (9 female, 8 male), 26 (39.4%) were surgeons (10 female, 16 male), and two (3%) were perfusionists (1 female, 1 male). Approximately one third of participants (n = 23 [34.8%]) were anaesthesia or surgical trainees (i.e. residents or fellows). Most participants practiced in Ottawa (n = 55 [83.3%]). Among surgeons (n = 26), 54% reported general surgery as their specialty (n = 14). The median age of participants was 35 years (IQR = 29–43).
| N (%) or Median (IQR) | |
|---|---|
| Registered Nurse (RN) | 19 (28.8%) |
| Surgeon (Post-graduate trainee) | 14 (21.2%) |
| Surgeon (Attending) | 12 (18.2%) |
| Anaesthesiologist (Post-graduate trainee) | 9 (13.6%) |
| Anaesthesiologist (Attending) | 8 (12.1%) |
| Perfusionist | 2 (3.0%) |
| Registered Practical Nurse (RPN) | 2 (3.0%) |
| General | 14 (53.8%) |
| Orthopedic | 3 (11.5%) |
| Urology | 3 (11.5%) |
| Gynecology/obstetrics | 1 (3.8%) |
| Neurosurgery | 1 (3.8%) |
| Otolaryngology | 1 (3.8%) |
| Plastic | 1 (3.8%) |
| Thoracic | 1 (3.8%) |
| Trauma | 1 (3.8%) |
| Toronto | 9 (13.6%) |
| Ottawa | 55 (83.3%) |
| Other | 2 (3.1%) |
| 35 (29–43) | |
| Female | 36 (54.5%) |
| Male | 30 (45.5%) |
*applies to surgery only (n = 26).
Overview of barriers and enablers identified within relevant domains
Barriers and enablers were identified across eight relevant domains ( behavioural regulation ; emotions ; environmental context and resources ; knowledge ; reinforcement ; skills ; social influences ; social/professional role and identity ). Fig 1 summarizes all of the barriers and enablers identified by participants across all relevant domains, with further details provided in S3 Appendix . The most commonly identified behavioural domains and themes are highlighted in Table 2 .

| Domain | Theme | Frequency of theme n participants (%) | |||
|---|---|---|---|---|---|
| Anaesthesia (n = 17) | Nursing (n = 23) | Surgery (n = 26) | Total across professions (n = 66) | ||
| Behavioural regulation | Communication practices or strategies (+) | 12 (71.0%) | 17 (73.9%) | 18 (69.2%) | 47 (71.2%) |
| People management (+) | 17 (100%) | 10 (43.5%) | 26 (100%) | 65 (98.5%) | |
| Emotions | Positive/negative emotions (+ -) | 15 (88.2%) | 18 (78.3%) | 22 (84.6%) | 55 (83.3%) |
| Environmental context and resources | Severity or type of case (+ -) | 12 (70.6%) | 5 (21.7%) | 23 (88.5%) | 40 (60.6%) |
| On-call/night shift (-) | 10 (58.8%) | 9 (39.1%) | 15 (57.7%) | 34 (51.5%) | |
| Resource-related challenges (-) | 8 (47.1%) | 23 (100%) | 22 (84.6%) | 53 (80.3%) | |
| Knowledge | Lack of awareness regarding best practices (-) | 10 (58.8%) | 15 (65.2%) | 14 (53.8%) | 39 (59.1%) |
| Shared definition of teamwork (+) | 15 (88.2%) | 15 (65.2%) | 24 (92.3%) | 54 (81.8%) | |
| Social influences | (Un)Familiarity with team members (+ -) | 10 (58.8%) | 10 (43.5%) | 18 (69.2%) | 38 (57.6%) |
| Hierarchies (-) | 13 (76.5%) | 17 (73.9%) | 24 (92.3%) | 54 (81.8%) | |
| Others’ personalities (-) | 14 (82.4%) | 22 (95.7%) | 24 (92.3%) | 60 (90.9%) | |
| Social/professional role and identity | Gender (-) | 13 (76.5%) | 21 (91.3%) | 25 (96.2%) | 59 (89.4%) |
| Teamwork is part of professional role (+) | 10 (58.8%) | 13 (56.5%) | 13 (50.0%) | 36 (54.5%) | |
| Conflicting professional norms/values/goals/perceptions (-) | 10 (58.8%) | 9 (39.1%) | 18 (69.2%) | 37 (56.1%) | |
*Theme identified by 50% or more of all participants and/or 50% or more of one professional group.
a Perfusionists (n = 2) were grouped with RNs (n = 19) and RPNs (n = 2) for the purposes of this summary.
(+) = enabler; (-) = barrier; (+ -) = viewed as enabler by some participants and barrier by others.
Cell frequency colour legend: darker to lighter shading = higher to lower frequencies
Most commonly identified themes within relevant domains
Key themes, domains and illustrative quotes are summarized in Table 3 and discussed below, in order of most to least frequently discussed.
| Theme (domain) | Illustrative quote |
|---|---|
| (+) People management (behavioural regulation) | “I, like some of my colleagues, probably resent a little bit being called, “Hey, anaesthesia,” you know? I have a name too and I think people just respond better to that”—Anaesthesiologist 1. |
| (-) Others’ personalities (social influences) | “…I mean, it’s hard to take your personality out of it, right? There’s one or two nurses, for example, who really rub me the wrong way. We just… we have personalities that, you know, we’d never be friends outside of work. Let’s just say that.”—Surgeon 22 |
| (-) Gender and other social identity factors (social/professional role and identity) | “…you know, strong female personalities are often perceived differently than strong male personalities. You know, whereas I think a man who has a really strong personality who’s, you know, maybe a little bit more rigid and not quite as flexible… which is often viewed as, you know, being themselves and, you know, they’re kind of a tough guy but they’re a leader, whereas I think where women demonstrate some of those same behaviours, they’re thought of as bitchy or difficult and it’s just that same behaviour be framed in a different context. So, I think in some ways it can be a little bit harder to be a woman and be respected as a leader without coming across as being difficult.”–Surgeon 9 “Being Asian, you know, being an Asian girl, and I look young. Definitely, I’m not treated the same as other people… I just… so I know what I’m walking into, and I’m not going to get upset about it, because it’s just a fact now that’s what I’m going to get most of the time…”–RN 1 |
| (+ -) Emotions (emotion) | “I remember working with one of the surgeons who was just very demeaning and very demanding… it’s hard to put into words but I found that that was really hard because everyone was kind of scared all the time, and tiptoeing around… that’s not great because people are kind of in an environment of fear and that’s not the best for the patient, right?”–Surgeon 2 |
| (-) Hierarchies (social influences; environmental context and resources) | “…the stereotypical situation is you have a medical student or a PGY1 who’s like, five minutes into their training, and they sort of walk in like, ‘I’m the doctor, you’re the nurse!’ And you have a nurse that’s been in practice for 30 years and is fantastic and really knows their stuff. And there’s a bit of a power struggle there because, I mean, technically, the doctor is, quote unquote, ‘in charge’. But, that being said, that nurse knows a whole lot more. And so, when you have people that feel the need to exert their expertise or sort of show their position in a social hierarchy, I think that makes the team dynamic much more difficult.”–Surgeon 18 “[our breakroom is] more around the OR, but I find that we don’t really have one common space where we all hang out before or after or in-between ORs… in general anyways. There’s the surgeon’s area and then there’s a separate nursing area. I don’t necessarily know why there is or needs to be that distinction. And where does housekeeping hang out? You know what I mean?”–Surgeon 5 |
| (-) Resource-related challenges (environmental context and resources) | “So lately we have a lot of equipment issues, for example, so when the equipment’s missing, the surgeon’s pissed because they don’t have the right things they need and who are yelling at you, “hey, Barbara, where’s the blah blah.” And it’s not Barbara’s fault that she doesn’t have it but… so yeah… You can have a great team that’s really working hard and really rolling well, the atmosphere’s great but if there’s a whole bunch of equipment problems, that can have a huge impact on the day and people’s morale and then all of a sudden you see the teamwork getting a little shakier and a little more rocky and all the pieces aren’t playing quite as well.”–Surgeon 6 “They [surgeons] often think it’s more related to incompetency but they also don’t realize that, at least in my current place right now, our training is very bad. Our orientation is really short because we’re short staffed, so they’re cutting our training in half. You know, it takes time to be familiar with a procedure. So, if you’re new in the OR it’s going to take a number of years. So, I think for them to be empathetic and realizing that and not raising their voice and understanding, okay well this is what I need next, then it’s fine, just communicate that. You know, all you got to do is just communicate it.”–RN 5 |
| (+) Shared definition of teamwork (knowledge) | “I would [define teamwork as] everyone working towards a common goal and a common goal being a good outcome for the patient.”–Surgeon 7 |
| (+) Communication practices or strategies (behavioural regulation) | “I like to ask a lot of questions… So, when I see people, I like to clarify things. I like to repeat things to make sure that there’s no errors. And I like to include people when decisions are made. And sometimes you have to go out of your way to do some of those things.”–RN 15 |
| (+ -) Severity or type of case (environmental context and resources) | “Yes, actually it’s funny. When it is an emergency situation, I find the communication’s a lot better because I think the surgeon realizes we don’t know exactly what they need. And, for some reason, for elective cases they have this impression that we know exactly what they want at all times. It’s like they’ve written down like a detailed instruction booklet for the case and we’re kind of confused and… I mean I think there needs to be more current communication each day. Like but for emergency situations, I think it’s actually a lot better.”–RN 6 |
| (-) Lack of awareness of best practices (knowledge) | “… sorry I’m not really aware of what’s best practice.”–RN 17 |
| (+ -) Familiarity (social influences) | “I would add a little insight into saying that I think it’s easy now because I’ve been here for six years and I know everybody. And I work at the [campus name], very rarely I take call at the [campus name] and there I actually find it a little bit challenging because I don’t know people. People don’t know me. So it’s hard when you don’t… and people kind of inherently trust you as the surgeon but it’s not really the same when they don’t know you, you know, or… so I think in those moments it’s actually quite challenging when you don’t know your team members quite as well.”–Surgeon 1 |
| (-) Conflicting professional norms/values/goals/perceptions (social/professional role and identity) | “I think everyone has the same global objective, but people might have different attributes of what they think makes an effective team. But that might almost be like the discrepancies in what their individual agendas are. Like, for example, like a surgeon might be really concerned about like doing something a particular way but maybe the anaesthetist is more worried about their time under GA being shorter. Overall both of them care about the patient’s well-being but because they have different specific agendas they might not share like the same focus as their own. Things could kind of misalign there.”–Surgeon 4 |
| (+) Teamwork as part of professional role (social/professional role and identity) | “I think because it’s just so ingrained in you as a nurse in general, like even from your training in nursing, like in university or college, it’s ingrained in you that, you know, nurses are teams, you work as a team..”–RN 9 |
| (-) On call/night shift (environmental context and resources) | “…on the day you’ve been up all night, and still working the full next day, you’re not as enthused with teamwork, you’re more just trying to survive through the day and then go”—Surgeon 13 |
People management (n = 65 [98.5%]; behavioural regulation )
The most common theme identified across participant responses was the role of “people management” in facilitating teamwork. Managing the people in the room was reported by 100% of anaesthesiologists and surgeons (n = 17, n = 26) to facilitate teamwork compared to less than 50% of nursing staff (n = 10). Participants identified a variety of strategies that they would often use in this regard, ranging from simply “being nice” to others to actively building relationships. As part of these strategies, participants emphasized the importance of using everyone’s names (e.g. writing down everyone’s name on a piece of paper in order to remember it).
Others’ “personalities” (n = 60 [90.9%]; social influences )
The influence of others’ “personalities” was frequently cited by participants as a barrier to teamwork in the OR. Participants acknowledged that there are certain team members who do not always work well together on a personal level. Faced with these situations, many participants expressed that they would try to adjust their behaviour or approach in the OR according to the “personalities” on the team that day. This could be challenging, however, when working with “difficult personalities” and participants expressed that there are certain individuals who are “just difficult to work with” (Anaesthesiologist 8) and who “don’t play nice with others” (Anaesthesiologist 15). Personality was also spoken about as a factor separate from skill level or professional role, which “spills over into every aspect of care” (Perfusionist 2).
Gender and other social identity factors (n = 59 [89.4%]; social/professional role and identity )
The third most common theme highlighted by participants was gender. The role of gender in the OR appeared to be particularly recognized among surgeons, with all but one discussing the influence of their own gender on teamwork or their observations about how others experience challenges related to gender (n = 25 [96.2%]). Several participants also acknowledged the “privilege” they experienced as white male physicians, whereby they often reported that they had an “easier” time in the OR in terms of obtaining respect, demonstrating leadership, and maintaining positive interactions. Conversely, team dynamics could be different when a female physician asserts leadership, and this was recognized by both male and female physicians. Many female participants also expressed how other elements of their social identity intersected with gender to shape their experiences in the OR (e.g. being female and Asian). Based on their social identity characteristics, participants expressed that they were often perceived by others as less competent and this placed strain on relationships within and across professions. Frequently, communication practices, perceptions of leadership, and acts of followership were reported by participants to vary depending on the social identities of the individuals in the room.
Emotions (n = 55 [83.3%]; emotions )
Emotions were described as both potential barriers and enablers of teamwork. In particular, several negative emotions associated with fear were noted to impede teamwork. Among the emotions discussed by participants, stress, being in a “bad mood”, or feeling scared of others, were indicated as barriers to teamwork while positive emotions were viewed as enablers of effective teamwork by participants. Participants also noted that the actions of others could influence their own emotions. One Registered Nurse shared that if a surgeon was yelling at them, it would cause them to feel afraid and subsequently withdraw from effective teamwork behaviours. Of note, 18 (27.3%) participants explicitly mentioned feeling scared, fearful, or intimidated with regard to interpersonal interactions in the OR, and this was primarily in reference to the dynamic between nurses and surgeons or between surgical residents and staff surgeons. Overall, these emotions were felt to be detrimental to patient care.
Hierarchies (n = 54 [81.8%]; social influences; environmental context and resources )
Participants described how various social hierarchies could affect teamwork, including conflicts between professional status and years of experience, such as a first-year resident challenging a nurse with 30 years of experience. Related to hierarchies, participants discussed how physical separation of professions outside of the OR (e.g. having separate lounges) further impacted interprofessional relationships and could reproduce interprofessional distinctions.
Participants also identified that hierarchies could be maintained within professional groups. One example was provided by an RN who described a new checklist introduced by management that “totally segregated” the nursing team by specifying “lead nurse, nurse number 2 and then RPN… [with] rules for each person.” (RN 6). Different meetings between different nursing and support team members (e.g. RNs, RPNs, orderlies) were also reported to cause divisions.
Resource-related challenges (n = 53 [80%]; environmental context and resources )
Resources, such as staffing and equipment issues, were identified by participants as barriers to teamwork. Notably, 100% of nursing staff (n = 23) and 85% of surgeons (n = 22) considered resource-related challenges to be a barrier to teamwork compared to 47% of anaesthesiologists (n = 8). Many tensions between nursing staff and surgeons were attributed by both groups to these issues.
Shared definition of teamwork (n = 54 [81.8%]; knowledge )
A key enabler for teamwork identified from participant responses was that most team members defined teamwork in the same way. Specifically, teamwork as spoken about as “working toward a common goal”, with the common goal being patient safety or a good outcome for the patient.
Communication practices or strategies (n = 47 [71.2%]; behavioural regulation )
Participants discussed a wide variety of communication practices or strategies which they used to facilitate teamwork. Examples included: asking questions, explaining actions out loud, expressing concerns in advance, including all team members in communications, speaking loudly, and calling for a pause or time-out.
Severity or type of case (n = 40 [60.6%]; environmental context and resources )
Participants highlighted clinical acuity as influencing teamwork, but there was variation in whether this was viewed as a barrier or enabler to teamwork. Some participants reported that teamwork improved during emergent cases, while others indicated that teamwork deteriorated with heightened urgency.
Lack of awareness of best practices (n = 39 [59.1%]; knowledge )
Nearly 60 percent of participants reported that they were not aware of any best practices for teamwork in the OR. Participants reported that teamwork “was not emphasized at any point” (Perfusionist 1) during their training and that they had not experienced anything “structured or formulated” (Surgeon 5). Teamwork was also spoken of as learned “on the job” and from mentors, rather than as a trainee. Participants expressed the desire for continuing professional education related to teamwork that would specifically bring the different OR professions together. As one surgeon explained, “you never really know” how you are perceived by others, and it is important to have feedback from other team members in addition to having simulation sessions with “the whole team practicing”.
Familiarity (n = 38 [57.6%]; social influences )
For effective teamwork to occur, over half of participants cited the importance of knowing other team members. Participants reported challenges when working in an OR with unfamiliar team members and revealed that there are different levels of trust depending on whether team members know each other or not.
Conflicting professional norms/values/goals/perceptions (n = 37 [56.1%]; social/professional role and identity )
Participants discussed how different professional socialization experiences and structures could pose challenges for teamwork. For example, “what would be leadership from a nursing perspective would be very different than leadership from a physician perspective, based on their roles and their training.” (Anaesthesiologist 2). Participants also acknowledged that there are “conflicting benefits” for each sub-team, such as the pressure for surgeons to move on to the next case while “from a union perspective” nurses are entitled to “breaks and lunches”, and that can put a case on hold (Surgeon 4).
Teamwork as part of professional role (n = 36 [54.5%]; social/professional role and identity )
Many participants reported that they viewed teamwork as part of their professional role. Surgeons reported that teamwork was important to them because they are “leaders within the room” whereas anaesthesiologists viewed teamwork as important based on their simulation and crisis resource management backgrounds. Nurses reported that “you cannot really do your entire job without having your team with you and guiding you and helping you” (RN 17).
On call/night shift (n = 34 [51.5%]; environmental context and resources )
Many participants viewed being on call or working a night shift as challenging for teamwork Participants expressed that the dynamic changes between team members during these shifts, where the focus becomes more on getting through the case rather than trying to be a good team member.
Key themes in less relevant domains
Most participants reported that they made a conscious effort to engage in good teamwork ( intentions ) and that effective teamwork promoted positive outcomes for both patients (e.g. reduced complications) and clinicians (e.g. job satisfaction) ( beliefs about consequences ). Participants also generally viewed teamwork as important or desirable ( goals ) and reported that teamwork was something they put effort into and eventually became automatic over time ( memory , attention and decision processes ). The domains of optimism and beliefs about capabilities were not observed among participant responses.
This study identified barriers and enablers to effective interprofessional teamwork in the OR based on theoretically-informed interviews with a large sample of practicing OR healthcare professionals across several sites and specialties. Specifically, we obtained an interprofessional perspective of teamwork for surgical patient safety, which is important for taking a comprehensive approach to improving performance and outcomes in the OR. This sets our work apart from other studies of OR teamwork, which have been largely atheoretical, providing broad observations or suggestions for improving teamwork rather than specific and actionable information [ 14 , 18 ].
In this study, personality conflicts across the professions were often cited as a barrier to teamwork and participants acknowledged the difficulty of working with individuals that they would not associate with outside of the OR. Although personality conflicts were discussed within professions, they were most apparent across professions, with one group perceiving another as “difficult” (e.g., surgeon-nurse conflicts). This finding is consistent with other studies showing discrepancies in perceptions of teamwork quality and team members’ roles among participants of different professions [ 39 – 42 ]. We also found that despite sharing a common overall definition of teamwork, participants often revealed how the norms and structures of their individual professions conflicted, straining interprofessional relationships in the OR, and posing a risk to patient safety. It may be that while OR clinicians agree on the concept of “teamwork”, the concept of “team” may be different. As Frasier and colleagues found, different OR professions offer a different definition of who they considered to be on their “team” for a given operation [ 43 ]. For example, nurses considered other nurses and technologists to be on their team and anaesthesiologists considers anyone involved in the provision of anaesthetic care to be on their team [ 43 ]. Consequently, a key challenge with OR teamwork may be its conceptualization as profession-specific rather than truly interprofessional.
Elements of power and hierarchy appeared to be at the centre of these issues, and participants often referred to the challenges associated with their position within the OR hierarchy. It was evident that profession is just one aspect of status in the OR, as participants explicitly discussed how various social factors (e.g., gender, profession, level of experience) worked together to shape perceptions and experiences of teamwork in the OR. Consequently, teamwork interventions may need to consider the simultaneous influence of multiple hierarchies rather than solely addressing interprofessional relations. A recent systematic review of interventions to improve OR culture reported that improvement strategies could be categorized as briefings/debriefings, team-building exercises, educational campaigns, and checklists [ 44 ]. Addressing social hierarchies, such as those related to gender or race, was not described in any of these intervention strategies. This may help to explain why there have been only moderate gains in patient safety in recent years despite the proliferation of teamwork interventions [ 45 – 48 ] given the significance of several types of hierarchies reported by participants in our study. Promoting inclusive leadership from an equity and diversity perspective [ 49 ] may therefore be an important consideration for future teamwork interventions.
The physical separation of professions outside of the OR was pointed out by several participants in our study. Familiarity was also frequently discussed by participants as critical for effective teamwork and has been reported on in other studies. For example, Reeves et al . found that, often in the perioperative environment, hierarchy and separateness between physicians and nurses is “compounded by their spending periods of time in separate spaces completing profession specific tasks or engaging in conversations with members from their own professional group” [ 50 ]. Others noted that relationships between healthcare providers, however, can change in different times and places [ 51 ]. For example, evidence shows communication patterns between physicians and nurses varies by where it takes place and is often more effective in more casual areas [ 52 ]. Therefore, one way to reduce the complex and intersecting hierarchies within the OR environment is to increase familiarity with team members [ 53 ]. An interprofessional lounge may be one component of a future intervention which could allow healthcare providers of different professions to interact with each other more frequently outside of case-related group tasks in the OR, facilitating a collaborative team culture [ 54 ]. Creating a collaborative culture is not just about exchanging information, but also fostering collaborative interprofessional working relationships [ 53 ]. This is often best accomplished in more “neutral” areas, such as an interprofessional lounge, where hierarchy can be alleviated as providers engage in collegial, casual social interactions [ 55 ]. Overall, putting in place organizational structures that require interprofessional interaction and reduced hierarchy, where providers can get to know each other “as people”, is a recommended best practice for teamwork in healthcare organizations [ 56 ] resulting in better patient care [ 57 ] and improved well-being for staff [ 58 , 59 ]. In fact, a recent experimental study found that once clinicians were taken out of the workplace and put into a controlled setting, professional tribalism, hierarchical and stereotyping behaviours largely dissolved [ 60 ]. Yet, previous teamwork interventions for the OR have often overlooked the fundamental aspects of building collaborative relationships across social and professional and boundaries to overcome unconscious biases and professional silos [ 59 , 61 ].
Along with increasing familiarity among team members, it may also be valuable to teach team members strategies for recognizing and challenging unconscious biases related to gender, ethnicity, and additional social identity factors [ 62 ]. This could be accomplished through trainee education and continuing professional development curricula [ 62 ]. Teaching team members specific strategies to assist individuals in speaking up or challenging authority when needed [ 63 ], along with conflict and emotion-management techniques [ 64 ], could also be valuable. It is important to note, however, that whether individuals feel able to use these strategies and skills may depend on their social position (e.g. gender, level of experience, profession). Future research may wish to examine whether intervention effectiveness varies by these characteristics. In any case, it is clear that addressing multiple aspects of power and hierarchy will be important to the success of any teamwork intervention.
Quantitative research suggests that equipment-related issues are correlated with higher stress and lower teamwork, particularly for nurses [ 65 ]. Equipment issues were particularly relevant to nursing staff and surgeons in our study, further supporting the relevance of these issues to interprofessional teamwork. Participants in our study also revealed that resource-related challenges (e.g. equipment and staffing availability) could further create tension between professional groups. These system-level factors should be considered in intervention development in order to promote sustainability. Even if teamwork practices can be improved and hierarchies reduced among OR teams, teamwork issues may be likely to still arise if staffing and equipment needs are not addressed.
A lack of knowledge and training regarding best practices for teamwork was identified as a barrier to teamwork across professions. To overcome this barrier, it may be useful to create a teamwork protocol, drawing upon strategies identified by OR team members. For example, participants in this study identified numerous strategies they used to facilitate communication, to manage their own behaviour, and to manage interactions with others. Of course, it is important to note some professional variation was observed regarding people management, whereby physicians appeared to engage in this strategy more frequently than nurses. This may reflect perceived differences in role, power, and influence among these two groups [ 41 ]. Once again, a teamwork protocol may help to overcome these discrepancies and empower all team members to engage in specific behaviours and actions to facilitate teamwork and patient safety. In any case, enhancing knowledge and training regarding best teamwork practices may also help to reduce some of the other barriers identified by participants. For example, learned teamwork skills may be used to navigate personality conflicts or the presence of negative emotions and ultimately lessen the impact of these barriers.
Emotions were also reported to be a key factor influencing teamwork in the OR. Each of these themes may be useful starting points to explore in moving toward enhanced teamwork education, training and guidelines. Addressing these considerations may also be a useful aid to teams during high acuity cases and call shifts, which were challenging times for teamwork identified by participants.
Strengths and limitations
Although we achieved saturation, not all surgical specialties were represented, and most surgeons who participated practised general surgery. It will be important for future studies to determine whether there are variations in the themes reported here depending on the particular surgical specialty. Similarly, OR support staff, such as attendants, did not participate in the study and only two perfusionists participated. Consequently, this study cannot draw conclusions based on the experiences of OR professions outside of nursing, anaesthesia or surgery. Nevertheless, our study did include a balance of trainees and non-trainees and female and male healthcare professionals across these three professions. Most participants, however, were from an Ottawa-based hospital. Results may therefore not be representative of teamwork experiences in other hospitals or geographic locations. For example, there may be different norms and practices in different places related to power and hierarchy. These should be examined in future work.
Unlike other studies [ 20 , 18 ], we did not aim to understand teamwork in one specialty, but teamwork in general. A key strength of our study is its large interprofessional sample, comprehensive and theory-informed interview guide, and conceptual generalizability and transferability [ 66 ]. Not only were we able to obtain important insights about teamwork from participants of different OR professions, but also, we were able to identify how numerous factors work together to shape barriers and enablers. This includes the finding that power and hierarchy in the OR exist along numerous social lines. It will be important for future work to further explore the larger social and structural factors influencing what is experienced as a barrier or enabler, by whom, and why. Although the TDF is useful for identifying specific influences on healthcare professional behaviour in order to inform intervention development, there may be other models, theories and frameworks that may be applied in future work to better understand broader cultural and contextual influences on teamwork and the inter-relationship between individual, team, and environmental factors. Nevertheless, this study reprsesnts a first step toward providing the type of data needed to move toward more effective interprofessional teamwork interventions for the OR.
Our study identified key determinants of OR teamwork from an interprofessional perspective using a theoretically informed and systematic approach. Results suggest that achieving optimal teamwork in the OR may require a multi-level intervention that addresses individual, team and systems-level factors with particular attention to complex social and professional hierarchies.
Supporting information
S1 appendix, s2 appendix, s3 appendix, acknowledgments.
Sandy Lam, Karthik Raj, and Ilinca Dutescu for their assistance with coordinating the study.
Dr. Boet was supported by The Ottawa Hospital Anesthesia Alternate Funds Association and the Faculty of Medicine, University of Ottawa with a Tier 2 Clinical Research Chair.
Funding Statement
This study was supported by a grant from the Canadian Institutes of Health Research (CIHR): #384512. Dr. Boet was supported by The Ottawa Hospital Anaesthesia Alternate Funds Association.
Data Availability
- Search Menu
- Sign in through your institution
- Advance articles
- Editor's Choice
- Supplements
- French Abstracts
- Portuguese Abstracts
- Spanish Abstracts
- Author Guidelines
- Submission Site
- Open Access
- About International Journal for Quality in Health Care
- About the International Society for Quality in Health Care
- Editorial Board
- Advertising and Corporate Services
- Journals Career Network
- Self-Archiving Policy
- Dispatch Dates
- Contact ISQua
- Journals on Oxford Academic
- Books on Oxford Academic

Article Contents
Introduction, conflict of interest.
- < Previous
A mixed-methods study of the causes and impact of poor teamwork between junior doctors and nurses
- Article contents
- Figures & tables
- Supplementary Data
Paul O'connor, Angela O'dea, Sinéad Lydon, gozie Offiah, Jennifer Scott, Antoinette Flannery, Bronagh Lang, Anthony Hoban, Catherine Armstrong, Dara Byrne, A mixed-methods study of the causes and impact of poor teamwork between junior doctors and nurses, International Journal for Quality in Health Care , Volume 28, Issue 3, June 2016, Pages 339–345, https://doi.org/10.1093/intqhc/mzw036
- Permissions Icon Permissions
This study aimed to collect and analyse examples of poor teamwork between junior doctors and nurses; identify the teamwork failures contributing to poor team function; and ascertain if particular teamwork failures are associated with higher levels of risk to patients.
Critical Incident Technique interviews were carried out with junior doctors and nurses.
Two teaching hospitals in the Republic of Ireland.
Junior doctors ( n = 28) and nurses ( n = 8) provided descriptions of scenarios of poor teamwork. The interviews were coded against a theoretical framework of healthcare team function by three psychologists and were also rated for risk to patients by four doctors and three nurses.
A total of 33 of the scenarios met the inclusion criteria for analysis. A total of 63.6% (21/33) of the scenarios were attributed to ‘poor quality of collaboration’, 42.4% (14/33) to ‘poor leadership’ and 48.5% (16/33) to a ‘lack of coordination’. A total of 16 scenarios were classified as high risk and 17 scenarios were classified as medium risk. Significantly more of the high-risk scenarios were associated with a ‘lack of a shared mental model’ (62.5%, 10/16) and ‘poor communication’ (50.0%, 8/16) than the medium-risk scenarios (17.6%, 3/17 and 11.8%, 2/17, respectively).
Poor teamwork between junior doctors and nurses is common and places patients at considerable risk. Addressing this problem requires a well-designed complex intervention to develop the team skills of doctors and nurses and foster a clinical environment in which teamwork is supported.
Effective teamwork between healthcare professionals is recognized to be a critical element of patient safety and quality of care [ 1 ]. Research has consistently demonstrated that the nature of the collaboration between doctors and nurses is related to patient outcomes such as the duration of patient stay [ 2 ], patient mortality [ 3 ] and the occurrence of medication errors [ 4 ].
Effective team functioning in the healthcare environment is well understood. An effective healthcare team shares common aims and objectives, has clearly defined goals, has a functional team leader, communicates efficiently and effectively, is cohesive and comprises team members who are respectful of one another [ 5 ]. A review of the literature suggests that the key elements of effective doctor–nurse teamwork are: the quality of the collaboration, coordination, shared mental models, communication and leadership [ 6 ]. These elements of teamwork are discussed briefly below.
Collaboration can be defined as respect and goodwill between team members, and coordination requires team members to work together in order to effectively manage a situation [ 6 ]. Collaboration and respect have been found to be predictors of patient safety climate [ 7 ]. However, there is evidence to suggest that interprofessional collaboration is less valued by doctors than by nurses [ 8 ]. Collaboration and coordination are also clearly challenged in environments in which bullying and undermining behaviours are common. An endemic culture of bullying and undermining behaviour in the clinical learning environment has been recognized both in Ireland [ 9 ] and in other countries [ 10 ]. In a 2015 survey of Irish interns, 29% reported that they had ‘frequently’ experienced bullying and undermining behaviour [ 9 ]. In a 2014 survey of nurses in Ireland, 51.9% reported that they had experienced bullying—an increase of 13.4% when compared with the results from a similar survey in 2010 [ 11 ].
Shared mental models provide team members with a common understanding. These models allow the team members to form accurate explanations and expectations about the task and to co-ordinate their actions and behaviours [ 12 ]. Shared mental models are crucial for effective patient care [ 13 ] and are supported by clear and effective communication. Communication can be defined as the exchange of information, feedback or response, about ideas and feelings [ 12 ].
Leadership can be defined as the effective and dynamic management of the healthcare team to ensure optimal outcomes [ 6 ]. It is unsurprising that leadership behaviours support effective teamwork. However, the use of effective leadership behaviours can be a particular challenge in environments in which team members do not have positional authority to take a leadership role (e.g. junior doctors and nurses working together in ad hoc teams).
Although there is a substantial body of evidence demonstrating that poor teamwork between doctors and nurses in commonplace [ 7 , 9 , 11 ], there is considerably less research on the interface between very junior doctors and nurses. However, of all the interprofessional relationships in the hospital, this relationship is particularly important. The reason for this importance is that the first doctor to be called by a nurse to evaluate a sick patient is often the most junior. Effective teamwork between junior doctors and nurses is particularly critical to the care of acutely unwell patients to ensure that they are identified and effectively treated. Yet, there is evidence that these newly qualified doctors are ill-prepared to perform their duties [ 14 , 15 ]. Junior doctors often struggle with knowledge transfer, dealing with uncertainty, understanding their role and operating within medical team hierarchies [ 14 , 16–20 ].
The objectives of the research reported in this paper were to: (i) collect and analyse examples of poor teamwork between nurses and interns (the first year of postgraduate training for a doctor in Ireland); (ii) identify the failures in teamwork that contributed to poor teamwork and (iii) ascertain if specific types of teamwork failures are associated with higher levels of risk to patients. The purpose of the paper was to provide the information necessary to support the development of evidence-based interventions designed to improve teamwork between junior doctors and nurses.
Setting and ethical approval
Participants were recruited from two large teaching hospitals in the Republic of Ireland. Ethical approval was obtained from the participating hospitals.
Participants
The participants were 28 interns (male, n = 12 and female, n = 16) in their first year of clinical practice. The interns had a mean of 0.49 years of experience (SD = 0.03). Eight qualified nurses (all female) also participated. The nurses had a mean of 8.9 years of experience (SD = 3.36). A total of 20 of the interns, and all of the nurses were from 1 hospital, and 8 interns from the other participating hospital. All of the participants worked on either a surgical or a medical ward.
Interview procedure
Critical Incident Technique (CIT) interviews were carried out in November and December 2012 and November and December 2013. CIT interviews enable the researcher to understand the knowledge, skills and attitudes of the respondents by asking them to describe a challenging incident. The CIT interview process involves several stages: (i) selecting an appropriate incident; (ii) developing a detailed description of the specific events, using probing questions to understand the reasoning; (iii) exploring cues and rationales for the actions taken by members of the team and (iv) identifying the root causes of the incident [ 21 ]. In our study, participants were asked to describe an event, in which they had been involved, where nurses and interns had failed to work effectively as a team. They were asked to select an event that had occurred within the previous 6 months. Probing questions focused on the teamwork aspects of the event. The interviews were recorded using a digital audio recorder.
Sampling was carried out using judgement and snowball methodologies. The interviewing continued until new categories, themes or explanations stopped emerging from the data and the research team determined that data saturation had been reached. This required an iterative approach to sampling, data collection, analysis and interpretation.
Three interns and one nurse were trained to conduct CIT interviews by a psychologist (POC) practised in using this methodology. Experience of carrying out CIT interviews in other domains suggests that social desirability bias can be reduced if interviews are conducted ‘within-group’ [ 21 ]. Thus, interns interviewed interns, and nurses interviewed nurses.
Content analysis
Three psychologists (POC, AOD, SL) with backgrounds in occupational health psychology carried out the analysis. Of the 36 scenarios collected (28 from interns and eight from nurses), 3 scenarios were discarded because they were not concerned with poor teamwork between interns and nurses. The unit of analysis was each of the 33 remaining scenarios.
A deductive content analysis approach was taken to organizing and analysing the data [ 22 ]. Manser's framework for effective team function [ 6 ] was used to code the teamwork failures contained within the scenarios. For the purposes of our research, the psychologists developed categories and definitions of each aspect of poor teamwork. These were: In order to ensure that the categories were sufficiently internally homogenous and externally heterogeneous, the definitions were illustrated with exemplar behaviours derived from the interview data (see Table 1 ).
‘poor quality of collaboration’—failure to work with other team members in a trusting and respectful manner;
‘lack of coordination’—failure to work effectively as a team and coordinate to prioritize a patient's needs and/or tasks;
‘lack of shared mental models’—team members do not have a common understanding about required task and/or patient care;
‘poor communication’—lack of clear and open communication between team members and
‘poor leadership’—lack of explicit leadership resulting in a failure to demonstrate or uphold appropriate standards of patient-focused clinical care.
Definitions, exemplar behaviours and interview quotes for each teamwork factor
| Aspect of teamwork . | Definition . | Exemplar behaviours . | Examples from interviews . |
|---|---|---|---|
| Poor quality of collaboration | Fails to work with other team members in a trusting and respectful manner. | ||
| Poor leadership | Fails to lead the team, or demonstrate appropriate standards of clinical care. | ||
| Lack of coordination | Fails to work effectively as a team and coordinate to prioritize a patient's needs and/or tasks. | ||
| Lack of shared mental models | Team members do not have a common understanding about required task and/or patient care. | ||
| Poor communication | Lack of clear and open communication between team members. |
| Aspect of teamwork . | Definition . | Exemplar behaviours . | Examples from interviews . |
|---|---|---|---|
| Poor quality of collaboration | Fails to work with other team members in a trusting and respectful manner. | ||
| Poor leadership | Fails to lead the team, or demonstrate appropriate standards of clinical care. | ||
| Lack of coordination | Fails to work effectively as a team and coordinate to prioritize a patient's needs and/or tasks. | ||
| Lack of shared mental models | Team members do not have a common understanding about required task and/or patient care. | ||
| Poor communication | Lack of clear and open communication between team members. |
The three psychologists then used the framework to code the failures in teamwork contained within the scenarios. These codes represented the contributory factors that lead to poor team function within the 33 scenarios. Each of the scenarios was discussed among the researchers, and consensus reached about which contributing factors were applicable. In addition, quotes were selected based on whether they were representative of the research findings. The selection of the quotes was carried out by consensus between the researchers.
Risk ratings
Seven SMEs rated the risk to patients associated with each scenario. The SMEs were 4 doctors with a mean of 14.0 years of experience (SD = 5.7) and 3 nurses with a mean of 12.7 years of experience (SD = 5.0). All of the SMEs were involved in intern training.
The scenarios were presented to the SMEs in a random order using on-line survey software. The Irish Health Services Executive's (HSE) risk assessment tool [ 23 ] was used to generate the risk rating. For each scenario, the SMEs were asked to rate the potential impact of the event on patient safety from ‘negligible’ (1) to ‘extreme’ (5). The SMEs were also asked to rate the likelihood of other interns/nurses encountering a similar situation from ‘rare/remote’ (1) to ‘almost certain’ (5). The ‘impact’ and ‘likelihood of occurrence’ ratings from each SME for each scenario were then multiplied together to give an overall risk score. A mean risk score based on the ratings of the seven SMEs was then calculated for each scenario. A risk rating of five or less was considered ‘low-risk’, between 5 and 12 ‘medium-risk’ and greater than >12 ‘high-risk’ [ 23 ]. The risk ratings and the content analysis were carried out independently.
‘ Poor quality of collaboration ’ was the most commonly identified cause of poor teamwork within the scenarios. A total of 21 out of 33 scenarios involved this teamwork failure (see Tables 1 and 2 ). Although the nurses appeared to work well together, there was evidence of nurses ‘ganging up’ on the intern (see Example 1 from Table 1 ). The interns reported feeling compelled to perform a task in order to ‘ keep the nurses happy ’ rather than because they felt the task was clinically necessary for the patient.
There were also a number of examples of aggressive and/or undermining behaviours between interns and nurses (see Examples 2 and 3 in Table 1 ). Nurses complained that interns did not value their experience. The interns also showed a lack of respect for nurses' opinions and/or clinical judgement (see Example 3 in Table 1 ). Interns reported feeling pressure from many competing demands, but the challenges of dealing with these demands were unrecognized by the nurses.
‘ Poor leadership ’ was identified as a contributing factor in 14 of the 33 scenarios (see Table 2 ). Poor leadership was synonymous with a lack of patient-focused care. In these instances, the team failed to act in the best interest of the patient or to maintain appropriate standards of patient care (see Examples 4 and 5 in Table 1 ). The reason for this lack of patient focus was generally because the interns and nurses were distracted from caring for the patient as a result of their frustrations with each other. As a result, there were sometimes delays in patient care, and on occasion a nurse or intern refused to carry out a task for a patient in order to ‘punish’ the intern or nurse with which they had a disagreement.
Frequency and Fisher's exact test comparison of aspects of poor teamwork based on level of risk
| Aspect of poor teamwork . | All ( = 33) . | Medium risk ( = 17) . | High risk ( = 16) . | -Value . |
|---|---|---|---|---|
| Poor quality of collaboration | 21 (63.6%) | 13 (76.5%) | 8 (50.0%) | 0.16 |
| Poor leadership | 14 (42.4%) | 10 (58.8%) | 4 (25.0%) | 0.08 |
| Lack of coordination | 16 (48.5%) | 9 (52.9%) | 7 (43.8%) | 0.73 |
| Lack of shared mental models | 13 (39.4%) | 3 (17.6%) | 10 (62.5%) | 0.01 |
| Poor communication | 10 (30.3%) | 2 (11.8%) | 8 (50.0%) | 0.03 |
| Aspect of poor teamwork . | All ( = 33) . | Medium risk ( = 17) . | High risk ( = 16) . | -Value . |
|---|---|---|---|---|
| Poor quality of collaboration | 21 (63.6%) | 13 (76.5%) | 8 (50.0%) | 0.16 |
| Poor leadership | 14 (42.4%) | 10 (58.8%) | 4 (25.0%) | 0.08 |
| Lack of coordination | 16 (48.5%) | 9 (52.9%) | 7 (43.8%) | 0.73 |
| Lack of shared mental models | 13 (39.4%) | 3 (17.6%) | 10 (62.5%) | 0.01 |
| Poor communication | 10 (30.3%) | 2 (11.8%) | 8 (50.0%) | 0.03 |
There was no evidence of interns or nurses taking a leadership role in any of the scenarios, resulting in a ‘lack of leadership’ as a recurrent theme. They would ‘ask’ each other to carry out tasks, but there was little evidence of either group assuming a leadership role in situations of uncertainty.
Just under half of the scenarios were attributed to a ‘ lack of coordination ’ (see Table 2 ). Common themes in these scenarios were: interns carrying out tasks they did not feel competent to perform (see Table 1 , Example 6), nurses not helping the intern (see Table 1 , Example 7) and interns who were unable to respond in a timely manner to calls to review patients, as they were occupied with other patients (see Table 1 , Example 8). The most common reasons for the lack of coordination were attributable to nurses, and more senior doctors, being too busy carrying out other tasks to be able to help the interns.
Additionally, nurses and interns differed in their willingness to recourse to senior members to resolve a lack of coordination and obtain support and advice (see Example 8 in Table 1 ). There were 10 instances of the nurse disagreeing with how an intern behaved or was treating a patient. In ninety percent (90%) of these occasions, the nurse contacted a more senior member in order to address the disagreement. There were 12 instances in which the intern disagreed with how a nurse behaved or was treating a patient. On three (25%) of these occasions, the intern contacted a more senior member to resolve the difficulty. The difference between nurses and interns in terms of their willingness to involve a senior team member is statistically significant (OR = 27.0, 95% CI (2.34–311.2), P < 0.001).
‘ Lack of shared mental models ’ was identified as a causal factor in approximately a third of the scenarios (see Table 2 ). The ‘lack of a shared mental models’ was used to categorize those scenarios in which the interns' understanding of the situation and the actions necessary, differed from the nurses' understanding of the situation (see Examples 9–11 in Table 1 ). The most common scenario was where an intern or nurse believed a particular treatment or medication had been given when, in fact, it either had not been given at all or a different treatment or medication has been administered.
For the ten scenarios in which ‘ poor communication ’ was identified as a causal factor, the overarching issue involved a failure to share pertinent information about patient care between nurses and interns (see Table 1 , Examples 12–14). This included failures to share information about a patient's condition, whether a particular treatment had been started (or discontinued), and the passing on of requests from others.
The seven SMEs read each of the scenarios and rated the potential impact on safety and likelihood of occurrence. The resulting data are shown in Table 3 .
Distribution of SME impact on safety and likelihood of occurrence ratings for the 33 scenarios
| Impact . | Percentage (proportion of ratings) . | Likelihood . | Percentage (proportion of ratings) . |
|---|---|---|---|
| Negligible | 2.2% (5/231) | Rare/remote | 1.7% (4/231) |
| Minor | 19.9% (46/231) | Unlikely | 8.2% (19/231) |
| Moderate | 29.0% (67/231) | Possible | 40.7% (94/231) |
| Major | 36.8% (85/231) | Likely | 36.4% (84/231) |
| Extreme | 12.1% (28/231) | Almost certain | 13.0% (30/231) |
| Impact . | Percentage (proportion of ratings) . | Likelihood . | Percentage (proportion of ratings) . |
|---|---|---|---|
| Negligible | 2.2% (5/231) | Rare/remote | 1.7% (4/231) |
| Minor | 19.9% (46/231) | Unlikely | 8.2% (19/231) |
| Moderate | 29.0% (67/231) | Possible | 40.7% (94/231) |
| Major | 36.8% (85/231) | Likely | 36.4% (84/231) |
| Extreme | 12.1% (28/231) | Almost certain | 13.0% (30/231) |
a The denominator is derived from the 7 SME ratings for each of the 33 scenarios.
None of the scenarios emerged as low risk, 17 scenarios emerged as medium risk and 16 scenarios emerged as high risk (see Table 2 ). The inter-rater reliability of the risk rating was a Fleiss' κ of 0.66 (substantial agreement).
High- and medium-risk scenarios were compared to ascertain if there were differences in the contributory teamwork failures. It emerged that a significantly larger proportion of high-risk scenarios were attributed to ‘lack of shared mental models’ and ‘lack of communication’ than the medium-risk scenarios (see Table 2 ). There were no significant differences between the high- and medium-risk scenarios in terms of attributions of ‘poor quality of collaboration’, ‘poor leadership’ or ‘lack of coordination’ (see Table 2 ).
In the Irish healthcare system, the first doctor to be called by a nurse to manage an acutely unwell patient is typically the most junior doctor on the team. As such, effective teamwork between these healthcare professionals is crucial for patient safety and quality of care. The research reported in this paper identified poor quality of collaboration, poor leadership and lack of coordination, as the most common causes of poor teamwork between nurses and interns. Moreover, up to half of the incidents were considered to have high impact on patient safety and to frequently occur within the healthcare system.
Collaboration and mutual respect are critical to effective patient care [ 7 ]. However, poor quality of collaboration was the most common failure of teamwork identified in the scenarios. Our study showed that conflict and bullying is also a feature of the nurse/intern relationship, and that these behaviours interfere with patient-focused care. Interns and nurses have different, and sometimes competing, goals that can compromise team coordination [ 19 , 20 ]. Although the nurses on a particular ward work as a team, the intern tends to work more autonomously in a role that is poorly defined, and with limited support from more senior doctors [ 16 , 19 , 20 ]. As such, the interns in this study often felt isolated and unsupported. The interns' isolation was compounded by the fact that, unlike nurses, interns seem reluctant to involve more senior doctors in settling any disagreements. This is consistent with research that has found that junior doctors are unwilling to seek guidance and clinical support from seniors, or inform them when they are struggling [ 24 ].
Lack of shared mental models and poor communication between interns and nurses were associated with high levels of-potential risk to patients. In fact, both hospitals in which our research was carried out have introduced a physiological track and trigger system (PTTS) to support both communication and the sharing of mental models between healthcare professionals, this procedural approach does not appear to have been as effective as desired. A PTTS is used to identify patients at-risk for worsening outcomes (track) and ensure that these patients receive appropriate care (trigger). The system includes a procedural communication tool for healthcare professionals (called ISBAR) [ 25 ]. However, research on the attitudes of staff at these two hospitals to the PTTS found that interns cited the PTTS as a source of conflict between doctors and nurses. Interns reported that the system created an expectation by nurses that the intern would respond immediately to each call that was received, and that it allowed the nurse to offload responsibility for the patient onto the intern. Both nurses and interns indicated that there was also a need to reinforce the use of ISBAR [ 26 ].
Poor quality of collaboration, lack of leadership, lack of coordination, lack of shared mental models and poor communication have been identified as detrimental to effective team performance in health care [ 14 , 16 , 19 , 20 ]. Our study adds context to this evidence with regard to the nurse/intern relationship and expands upon previous research by using SMEs to generate risk ratings in order to identify the teamwork failures that have the greatest potential to result in patient harm. Using this methodology, it emerged that almost one half of the scenarios were considered to pose ‘high’ levels of risk to patients. Moreover, high-risk situations are more likely to be caused by poor situation awareness between team members and lack of communication. This evidence provides support for the development of targeted interventions to tackle the teamwork failures that pose the greatest risk to patients. Our research identifies a ‘lack of shared mental models’ and ‘lack of communication’ as teamwork problems which pose the greatest risk to patient safety. Thus, effective interventions designed to improve teamwork performance in these areas must be developed and evaluated.
Recommendations to improve teamwork
Taking a sociotechnical systems approach to poor teamwork between intern and nurses, it is possible to recommend a number of interventions: A consistent finding in articles on quality improvement in healthcare is that change is difficult to achieve [ 34 ]. Common reasons why interventions fail to have a long-term impact include a failure to: develop the interventions systematically; use best available evidence and appropriate theory; and understand the environment in which the intervention is to be applied [ 35 ]. Therefore, there is a need for a measured approach that incorporates behavioural change and implementation science. It is suggested that the UK Medical Research Council Complex Intervention Framework [ 36 ] be used to design appropriate interventions and planning policies that support the desired changes in behaviour [ 34 ]. Such an intervention will require collaboration between medical and nursing schools, as well as hospital-based senior doctors and nurses in order to produce a sustained change in teamwork between interns and nurses.
At a societal, cultural and regulatory level, increasing the resourcing of hospitals and employing a greater number of interns and nurses will reduce workload, and possibly levels of undermining and bullying behaviour [ 27 ].
At an organizational level, legislation, collective agreements and other regulatory agreements could be used to address the endemic culture of undermining and bullying behaviour [ 28 ]. Hospital-wide quality management systems have also been found to be associated with positive teamwork climate [ 29 ].
At a team level, increasing the level of support for interns by senior doctors and carrying out multidisciplinary team training, such as crew resource management, has been shown to improve teamwork and may improve the quality of junior doctor–nurse collaboration [ 30 , 31 ].
At an individual level, interprofessional shadowing (e.g. medical students spend time shadowing nurses [ 32 ]) has been shown to improve the understanding of the role and the responsibilities of each member of the team which may improve junior doctor–nurse relations.
At the work environment level there is a need for a better definition of the roles and responsibilities of a junior doctor [ 14 , 16–19 ] and more rigorous use of any existing PTTSs, and ISBAR.
At the patient level, simulation can provide a safe-learning environment in which interns and nurses can learn to work as an effective team, to care for complex simulated patients [ 33 ].
Limitations
In common with other qualitative research approaches, the CIT could be criticized due to subjectivity in the reporting or the analysis of the data. In order to mitigate these issues, a rigorous approach was taken to both the collection and analysis of the data. In addition, CIT could be criticized for lack of generalizability. Since the CIT is based on the analysis of incidents of poor teamwork it may not be representative of typical levels of collaboration between nurses and interns. There is certainly some possibility of this, but the ratings of the SME would suggest that at least half of the scenarios were a ‘likely’ or ‘almost certain’ occurrence. Other limitations were that nurses may have been underrepresented in the sample, resulting from the use of convenience and snowball sampling. Nevertheless, the findings from the study are in broad agreement with similar studies carried out in other countries [ 16 , 19 ].
Qualitative, as opposed to quantitative principles were used to determine the number of interviews that were necessary. Therefore, there is a possibility of Type II error in the analysis of differences between the high- and medium-risk scenarios. Future studies may use the data provided here as a basis for sample size calculations, such data were not available for this study.
Poor teamwork between nurses and junior doctors is not a new phenomenon. However, effective teamwork between junior doctors and nurses is crucial to patient safety and quality of care. Changes in both the delivery of healthcare and the clinical working environment mean that interprofessional teamwork has, and will continue to, become increasingly important to the delivery of safe and effective patient care. There is not a simple solution to improving teamwork. It requires a complex intervention that focuses on the development of the team skills of doctor and nurses, and fostering a clinical environment in which teamwork is supported.
This research was partially supported through funding from the Intern Education and Training Service Level Agreement, National Doctors Training and Planning and Health Services Executive.
None declared.
World Health Organization . Framework for action on interprofessional education and collaborative practice . Geneva, Switzerland , 2010 . www.who.int/hrh/resources/framework_action/en/ (2 June 2015, date last accessed) .
Dutton RP , Cooper C , Jones A et al. . Daily multidisciplinary rounds shorten length of stay for trauma patients . J Trauma Acute Care Surg 2003 ; 55 : 913 – 9 .
Google Scholar
Neily J , Mills PD , Young-Xu Y et al. . Association between implementation of a medical team training program and surgical mortality . J Am Med Assoc 2010 ; 304 : 693 – 700 .
Manojlovich M , DeCicco B . Healthy work environments, nurse-physician communication, and patients’ outcomes . Am J Crit Care 2007 ; 16 : 536 – 43 .
Mickan SM , Rodger SA . Effective health care teams: a model of six characteristics developed from shared perceptions . J Interprof Care 2005 ; 19 : 358 – 70 .
Manser T . Teamwork and patient safety in dynamic domains of healthcare: a review of the literature . Acta Anaesthesiol Scand 2009 ; 53 : 143 – 51 .
Manojlovich M , Kerr M , Davies B et al. . Achieving a climate for patient safety by focusing on relationships . Int J Qual Health Care 2014 ; 26 : 579 – 84 .
Braithwaite J , Westbrook M , Nugus P et al. . Continuing differences between health professions’ attitudes: the saga of accomplishing systems-wide interprofessionalism . Int J Qual Health Care 2013 ; 25 : 8 – 15 .
Irish Medical Council . Your training counts: results of the national trainee experience survey 2015 . http://www.medicalcouncil.ie/News-and-Publications/Reports/Your-Training-Counts-2015-pdf-.pdf (14 December 2015, date last accessed) .
Quine L . Workplace bullying in junior doctors: questionnaire survey . Br Med J 2002 ; 324 : 878 – 9 .
Sheehan M , McCabe TJ . Executive summary: INMO workplace bullying survey findings over the past four years (2010–2014) . www.inmo.ie/tempDocs/Executive%20Summary%20Bullying.pdf (20 May 2015, date last accessed) .
O'Connor P , Keogh I , Azuara-Blanco A . Teamwork and communication . In: Flin R , Youngson G , Yule S , (eds). Enhancing Surgical Skills: A Primer in non-Technical Skills . London : CRC Press , 2015 , 105 – 22 .
Google Preview
Burtscher MJ , Kolbe M , Wacker J et al. . Interactions of team mental models and monitoring behaviors predict team performance in simulated anesthesia inductions . J Exper Psy (Appl) 2011 ; 17 : 257 – 69 .
Tallentire VR , Smith SE , Skinner J et al. . The preparedness of UK graduates in acute care: a systematic literature review . Postgrad Med J 2012 ; 88 : 365 – 71 .
Illing J , Morrow G , Kergon C et al. . How Prepared are Medical Graduates to Begin Practice: A Comparison of Three Diverse UK Medical Schools . London : General Medical Council , 2008 .
Tallentire VR , Smith SE , Skinner J et al. . Understanding the behaviour of newly qualified doctors in acute care contexts . Med Educ 2011 ; 45 : 995 – 1005 .
Byrne D , O'Connor P , Lydon S et al. . Preparing new doctors for clinical practice: an evaluation of pre-internship training . Ir Med J 2012 ; 105 : 328 – 30 .
Weller J , Boyd M , Cumin D . Teams, tribes and patient safety: overcoming barriers to effective teamwork in healthcare . Postgrad Med J 2014 ; 90 : 149 – 54 .
Weller JM , Barrow M , Gasquoine S . Interprofessional collaboration among junior doctors and nurses in the hospital setting . Med Educ 2011 ; 45 : 478 – 87 .
Milne J , Greenfield D , Braithwaite J . An ethnographic investigation of junior doctors’ capacities to practice interprofessionally in three teaching hospitals . J Interprof Care 2015 ; 29 : 347 – 53 .
O'Connor P , O'Dea A , Melton J . A methodology for identifying human error in US Navy diving accidents . Hum Fac 2007 ; 49 : 214 – 26 .
Elo S , Kyngas H . The qualitative content analysis process . J Adv Nurs 2008 ; 62 : 107 – 15 .
Irish Health Service Executive . Risk assessment tool and guidance . Dublin : Quality and Patient Safety Directorate , 2011 . www.hse.ie/eng/about/Who/qualityandpatientsafety/resourcesintelligence/Quality_and_Patient_Safety_Documents/riskoctober.pdf (2 June 2015, date last accessed) .
O'Connor P , Keogh I , Ryan S . A comparison of the teamwork attitudes and knowledge of Irish surgeons and U.S. Naval aviators . Surg 2012 ; 10 : 278 – 82 .
De Meester K , Verspuy M , Monsieurs K et al. . SBAR improves nurse–physician communication and reduces unexpected death: A pre and post intervention study . Resuscitation 2013 ; 84 : 1192 – 6 .
Lydon S , Byrne D , Offiah G et al. . A mixed-methods investigation of health professionals’ perceptions of a physiological track and trigger system . BMJ Qual Saf 2015 . 10.1136/bmjqs-2015-00426 .
Johnson SL . International perspectives on workplace bullying among nurses: a review . Int Nurs Rev 2009 ; 56 : 34 – 40 .
Quinlan E , Robertson S , Miller N et al. . Interventions to reduce bullying in health care organizations: a scoping review . Health Serv Manage Res 2014 ; 27 : 33 – 44 .
Kristensen S , Hammer A , Bartels P et al. . Quality management and perceptions of teamwork and safety climate in European hospitals . Int J Qual Health Care 2015 . http://dx.doi.org/10.1093/intqhc/mzv079 .
O'Dea A , O'Connor P , Keogh I . A meta-analysis of the effectiveness of crew resource management training in acute care domains . Postgrad Med J 2014 ; 90 : 699 – 708 .
Clay-Williams R , McIntosh CA , Kerridge R et al. . Classroom and simulation team training: a randomized controlled trial . Int J Qual Health Care 2013 ; 25 : 314 – 21 .
Shafran DM , Richardson L , Bonta M . A novel interprofessional shadowing initiative for senior medical students . Med Teach 2015 ; 37 : 86 – 9 .
Kneebone R , Scott W , Darzi A et al. . Simulation and clinical practice: strengthening the relationship . Med. Educ. 2004 ; 38 : 1095 – 102 .
Grol RP , Bosch MC , Hulscher ME et al. . Planning and studying improvement in patient care: the use of theoretical perspectives . Milbank Q 2007 ; 85 : 93 – 138 .
Michie S , van Stralen MM , West R . The behaviour change wheel: a new method for characterising and designing behaviour change interventions . Implement Sci 2011 ; 6 : 42 .
Craig P , Dieppe P , Macintyre S et al. . Developing and evaluating complex interventions: the new Medical Research Council guidance . BMJ 2008 ; 337 : a1655 .
| Month: | Total Views: |
|---|---|
| December 2016 | 6 |
| January 2017 | 18 |
| February 2017 | 36 |
| March 2017 | 37 |
| April 2017 | 227 |
| May 2017 | 83 |
| June 2017 | 32 |
| July 2017 | 34 |
| August 2017 | 47 |
| September 2017 | 63 |
| October 2017 | 95 |
| November 2017 | 128 |
| December 2017 | 365 |
| January 2018 | 335 |
| February 2018 | 350 |
| March 2018 | 397 |
| April 2018 | 479 |
| May 2018 | 806 |
| June 2018 | 592 |
| July 2018 | 553 |
| August 2018 | 689 |
| September 2018 | 602 |
| October 2018 | 680 |
| November 2018 | 876 |
| December 2018 | 617 |
| January 2019 | 587 |
| February 2019 | 604 |
| March 2019 | 724 |
| April 2019 | 1,110 |
| May 2019 | 920 |
| June 2019 | 549 |
| July 2019 | 687 |
| August 2019 | 675 |
| September 2019 | 668 |
| October 2019 | 730 |
| November 2019 | 687 |
| December 2019 | 514 |
| January 2020 | 543 |
| February 2020 | 524 |
| March 2020 | 501 |
| April 2020 | 723 |
| May 2020 | 390 |
| June 2020 | 504 |
| July 2020 | 404 |
| August 2020 | 418 |
| September 2020 | 532 |
| October 2020 | 651 |
| November 2020 | 665 |
| December 2020 | 547 |
| January 2021 | 478 |
| February 2021 | 447 |
| March 2021 | 636 |
| April 2021 | 581 |
| May 2021 | 437 |
| June 2021 | 324 |
| July 2021 | 295 |
| August 2021 | 279 |
| September 2021 | 277 |
| October 2021 | 862 |
| November 2021 | 970 |
| December 2021 | 290 |
| January 2022 | 385 |
| February 2022 | 405 |
| March 2022 | 509 |
| April 2022 | 510 |
| May 2022 | 454 |
| June 2022 | 308 |
| July 2022 | 305 |
| August 2022 | 328 |
| September 2022 | 369 |
| October 2022 | 782 |
| November 2022 | 729 |
| December 2022 | 414 |
| January 2023 | 470 |
| February 2023 | 420 |
| March 2023 | 599 |
| April 2023 | 611 |
| May 2023 | 560 |
| June 2023 | 362 |
| July 2023 | 336 |
| August 2023 | 280 |
| September 2023 | 421 |
| October 2023 | 608 |
| November 2023 | 621 |
| December 2023 | 330 |
| January 2024 | 446 |
| February 2024 | 326 |
| March 2024 | 558 |
| April 2024 | 414 |
| May 2024 | 435 |
| June 2024 | 253 |
| July 2024 | 169 |
| August 2024 | 131 |
Email alerts
Citing articles via.
- Recommend to your Library
Affiliations
- Online ISSN 1464-3677
- Print ISSN 1353-4505
- Copyright © 2024 International Society for Quality in Health Care and Oxford University Press
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
- Real Life Examples of Successful Teamwork [9 Cases]

Instead of retelling the same old stories about the best teamwork practices from companies such as Google, Chevron, or the Southwest airlines (which don’t really help when you have a small-to-medium team), we decided to find real-life examples of successful teamwork.
We asked everyday entrepreneurs, CEOs, and HR managers one simple question:
How did you improve teamwork in your organization?
Here are the best 9 examples we came across.
3-step onboarding

Developing teamwork should start as soon as the new employee walks through the door. According to Lauren McAdams , career advisor and hiring manager at ResumeCompanion.com , the most successful method for creating excellent intra-team relations was instilling a sense of teamwork early on in the onboarding process.
”While we do experiment with different team-building measures, there are three that have become common practice:
First, during onboarding, we have new employees shadow an experienced “coach” who is tasked with helping their integration into the team. After the initial phase, we assign the new employees to shadow other people so they get to have more than one “coach”.
Next, when we begin a new project, I personally assign mini-teams to handle those projects. These smaller units are often comprised, in part, of employees who haven't had a chance to work together. This way, new hires get an opportunity to work and develop relationships with everyone they collaborate with.
And finally, leadership rotates on these projects so different people have a chance to test their leadership skills. Also, since project teams always have different people on them, everyone in the company gets to know each other at some point by working together. This level of exposure and collaboration resulted in very strong teamwork at our company.”
Role switching

Some organizations encourage their employees to walk a mile in someone else's shoes. Lee Fisher , an HR manager at Blinds Direct , says that successful teamwork should be based on solidarity, respect, communication, and mutual understanding. With that in mind, his company has been organizing a series of team-building events over the years.
“Our most unconventional event to date was the 'Role Switch'. It was launched across our web and marketing department. In the event, each team member switches roles with a colleague. Usually, team members work together closely but they don’t really understand the complexities of other person’s role.
Spending a day in your colleague’s shoes highlights their efforts, which brings more understanding and respect for one another. The 'Role Switch' was a huge success: it brought the team closer together and made people more considerate of other's workloads and requirements .”
Cross-training

Sharing experience with your peers is important, but recognizing where they can best help you improve is even more important. According to Steven Benson , founder, and CEO of Badger Maps , his company has benefited from one self-initiated cross-training session which resulted in an increase in both teamwork and productivity.
”An example of successful teamwork at our company was when the customer relation department put together an initiative of cross-training and specializing team members for different roles. After deciding who will focus on what, the group sat down and taught one another what they would need to become the expert in their respective area.
Because people were cross-trained, they had a broader set of skills they could use to handle customer interaction - which resulted in fewer hand-offs. This not only enhanced teamwork and productivity, but also improved customer satisfaction. Everyone worked as a team and covered for one another, which made everything move smoothly and quickly."

The Big Book of Team Culture
*Enter your email address and subscribe to our newsletter to get your hands on this, as well as many other free project management guides.
We weren't able to subscribe you to the newsletter. Please double-check your email address. If the issue persists, let us know by sending an email to [email protected]
Newsletter subscribers can download all free materials
Scheduled breaks and self-reflection

Publicly reflecting on achievements increases everyone’s morale. Bryan Koontz , CEO of Guidefitter , considers teamwork to be more than just brainstorming ideas or helping a colleague on a project - it’s about fostering a culture of trust and respect.
“A few ways we cultivate an environment of trust and respect is through meetings, or rather "breaks", that don't necessarily focus on work. By scheduling “break” times in our calendars, we allow our employees to talk, relax, and discuss the ins-and-outs of their days.
We also strengthen our teams through brief weekly meetings with the entire office: each Wednesday morning we huddle up to recap the past week, with each employee sharing one professional and one personal "win". This encourages everyone to pause for self-reflection on their achievements, often serving as motivation to their peers while forging a bond among our team members.”
Team traditions

Members of jelled teams have a strong sense of identity and often share traditions like getting together for a drink after work. According to Katerina Trajchevska co-founder and CEO of Adeva , establishing team traditions is the foundation upon which teamwork is built.
“Rather than using one particular method for strengthening our team, we focus on creating an environment that fosters team spirit and communication. We organize after hours drinks and hangouts, and develop a culture that encourages everyone to speak up and take part in the big decisions for the company.
Team traditions can do wonders, no matter how trivial they seem: we have a team lunch every Friday, celebrate birthdays and other important dates, and celebrate one of our national holidays together. All of this has contributed to a more cohesive and a close-knit team.”
Unconventional business meetings

Some companies use their business meetings to improve teamwork within the organization by making them fun and laid-back. James Lloyd-Townshend , CEO of Frank Recruitment Group believes that bringing teams together in an informal environment improves teamwork, strengthens bonds, and bolsters morale - which is why he decided to spice up the company’s monthly meetings.
”One unusual method we’ve introduced is “First Thursdays”: we start off our monthly business meetings with a business review, promotions, and awards - and then move on to an open bar event.
Apart from “First Thursdays,” we also have “Lunch Club”: another monthly event where employees enjoy an all-expense-paid afternoon to celebrate their success and enjoy fine dining and have fun with their colleagues.
However, the most popular team building method we employ is our incentivised weekends away. Our top-performing consultants get the chance to travel to major cities such as London, New York, and Miami as the rewards for their hard work.”
Peer recommendations

Some companies are building teamwork through peer recognition. Jacob Dayan , a partner, and co-founder of Community Tax said that encouraging employees to be active participants in recognizing their peers has proven to be quite a powerful motivational tool.
”I ask employees to share or report instances when someone on their or another team has been particularly helpful or has gone above and beyond their call of duty. After we thank the contributing employee for their input, we make sure the employee being acknowledged knows the source of information. Having employees “nominate” their peers for recognition has the additional bonus of bringing them closer together and building camaraderie with long-term productivity benefits.”
However, Mr. Dayan is well aware that peer reports and nominations can be driven by personal feelings (positive as well as negative), and can give an unrealistic representation of certain employee's contribution.
”Personal relationships, both close and less so, are an important consideration when pursuing this approach, which is why we do not hand out recognition without validating the worthiness of the employee's contribution. We ask the appropriate manager to review the submission and keep an eye on it over time, just to make sure there are no dubious activities.”
Conflict resolving

Successful teamwork happens when members of a group trust each other, are comfortable expressing themselves, and deal effectively with conflict, according to Laura MacLeod , a licensed social worker specialized in group work, an HR consultant, and a mastermind behind “From the inside out project” .
”Many companies think that team building is about company picnics, happy hours, and other fun events. These things are fine, but they don't address the real issues people face when they have to work together. Going out for a drink with someone you can't get along with will be just as uncomfortable and awkward as trying to finish a project with that person - the only difference is having alcohol as a buffer.”
According to Laura, certain team-building exercises can help individuals overcome both intragroup and personal conflicts .
“Choose simple activities that help build cohesion and trust amongst team members. For example, you can use “Pantomime in a circle” exercise: without using words, pass an imaginary object (a bucket of water or a ball) around the circle; the point of the exercise is for group members to rely on each other to complete the activity.
When it comes to personal misunderstandings, you might want to choose an activity where you are actually allowed to yell at a person. So, pair off people and have them repeat opposing sentences (such as it’s hot/it’s cold) back and forth - going from soft to very loud. This will allow people to get out strong emotions in a non-threatening way, and blow off some steam in the process.”
"Spotless" team-building exercise

Dmitri Kara , a tenancy expert at Fantastic Cleaners , shared with us a team-building exercise his team uses to increase cooperation and efficiency.
”Everybody in the office has to simultaneously perform a 2-to-5-minute cleaning routine (like wipe their desk, keyboard, monitor, shelves). But there’s a catch: the tools are limited. For example, make everybody wipe the dust off their desks at the same time but provide only 2 sprayers and 1 roll of paper towel (if your team has 10 members)-. Scarcity will encourage people to share and help each other.”
Besides providing obvious benefits (like a cleaner working environment), Dmitri says this team building activity boosts organization, improves long-term productivity, and develops a sense of morale, discipline, and shared responsibility. He even shares how the exercise came into being:
”At first it was not really a dedicated exercise. The first time we did it all together, it was because of a video shoot. But since it felt good, a few days later somebody said, "let's do that again". And that's where the whole thing came to be.”

ActiveCollab 2021 Calendar
Other posts in the series on the big book of team culture.
- Tips To Take Better Meeting Notes
- How To Be a Good Team Leader
- How To Deal With a Toxic Coworker
- How to Create Organizational Culture
- Characteristics of a Productive Team
- Group vs Team [Differences, Comparison, Transformation]
- Belbin Team Roles: Theory and Practice
- High Performing Teams: What Are They and How Do I Build One?
- All Leadership Theories in Under 15 Minutes
- What Is Teamwork Actually?
- Organizational Culture and Its Impact on Team Performance
- Types of Teams [Advantages and Disadvantages]
Start your trial today, free for 14 days ! Onboard your team, plan, collaborate, organize your work, and get paid.
By signing up you are agreeing to the ActiveCollab Terms of Service & Privacy Policy.

Choose your favorite topics and we’ll send our stories from the tech front lines straight to your inbox.
Unsubscribe at any time * ActiveCollab Privacy Policy
Just a second
Awesome! Thank you for subscribing to our newsletter.
Oops, something went wrong! Please try again later.
Related Articles

We detected that you already have an ActiveCollab account
You can log in to an excisting account or you may start a new one
Great, just a few seconds and you're in.
All done! Redirecting you to your account.
We've sent you an email to confirm that it's you. Please check your email to complete the trial account creation.
Sorry, we could not create an account for you at this moment. Please double check your email address. If the issue still persists, please let us know by sending an email to [email protected]
- SUGGESTED TOPICS
- The Magazine
- Newsletters
- Managing Yourself
- Managing Teams
- Work-life Balance
- The Big Idea
- Data & Visuals
- Reading Lists
- Case Selections
- HBR Learning
- Topic Feeds
- Account Settings
- Email Preferences
The Secrets of Great Teamwork
- Martine Haas
- Mark Mortensen

Over the years, as teams have grown more diverse, dispersed, digital, and dynamic, collaboration has become more complex. But though teams face new challenges, their success still depends on a core set of fundamentals. As J. Richard Hackman, who began researching teams in the 1970s, discovered, what matters most isn’t the personalities or behavior of the team members; it’s whether a team has a compelling direction, a strong structure, and a supportive context. In their own research, Haas and Mortensen have found that teams need those three “enabling conditions” now more than ever. But their work also revealed that today’s teams are especially prone to two corrosive problems: “us versus them” thinking and incomplete information. Overcoming those pitfalls requires a new enabling condition: a shared mindset.
This article details what team leaders should do to establish the four foundations for success. For instance, to promote a shared mindset, leaders should foster a common identity and common understanding among team members, with techniques such as “structured unstructured time.” The authors also describe how to evaluate a team’s effectiveness, providing an assessment leaders can take to see what’s working and where there’s room for improvement.
Collaboration has become more complex, but success still depends on the fundamentals.
Idea in Brief
The problem.
Teams are more diverse, dispersed, digital, and dynamic than ever before. These qualities make collaboration especially challenging.
The Analysis
Mixing new insights with a focus on the fundamentals of team effectiveness identified by organizational-behavior pioneer J. Richard Hackman, managers should work to establish the conditions that will enable teams to thrive.
The Solution
The right conditions are
- a compelling direction
- a strong structure
- a supportive context, and
- a shared mindset
Weaknesses in these areas make teams vulnerable to problems.
Today’s teams are different from the teams of the past: They’re far more diverse, dispersed, digital, and dynamic (with frequent changes in membership). But while teams face new hurdles, their success still hinges on a core set of fundamentals for group collaboration.
- Martine Haas is the Lauder Chair Professor of Management at the Wharton School and Director of the Lauder Institute for Management & International Studies at the University of Pennsylvania. She holds a PhD from Harvard University. Her research focuses on collaboration and teamwork in global organizations.
- Mark Mortensen is a professor of organizational behavior at INSEAD and for over 20 years has studied and consulted on collaboration and organization design, with a focus on hybrid, virtual, and globally distributed work. Mark publishes regularly in Harvard Business Review , MIT Sloan Management Review , and INSEAD Knowledge, and is a regular fixture in popular press outlets like the BBC, the Economist , the Financial Times , and Fortune .
Partner Center
| Intelligent strategy by DESIGN | ||
Recent Posts
- Successful Mentoring Programs
- Human Resources & Learning & Development – Are You Providing Training Programs for your Senior Leaders?
- What Change Initiatives(Projects) Will You Launch in 2020?
- Hey Leaders – How about the impact of change on you?
- Providing Opportunities for Employees When Career Paths Do Not Exist
- Providing Feedback that Makes Sense!
- Why Emotional Intelligence Matters for Leaders
- Helping New Managers Succeed
A Mini Case Study: What’s Wrong With This Team – Part II
Read Part I of the mini case study.
What may be some of the primary reasons for the team feeling as they are?
There are any number of issues that could be happening. The members may not understand what it means to be part of a team, may have had poor experiences on past teams, or even may have so much going on that they feel they cannot take on one more assignment. Certainly there is no commitment to teamwork or to the team as a whole. There are so many reasons as to why the team members may feel as they do. In order to understand the reasons for the team feeling as they do, it is a good practice to reach out to the team members individually to understand their concerns in more detail. Understanding their past experiences working in teams – whether at this organization or another – will help in moving them forward. A better understanding of the team members enables for getting to the root of the problem and to make changes/adjustments to correct it.
What should be done at this point?
The team leader needs to set up individuals meetings with each team member to:
- Discuss their concerns
- Understand their past experiences working on the team
- Determine their commitment to teamwork in general and in particular for this project
Once the team leader has met with each team member individually, a team meeting (ideally in person) should be held with a focus on:
- Team building activities
- Sharing the objectives of the project
- Set team goals (in line with the objectives of the project)
- Determine roles and responsibilities on the team
- Resolving conflicts on the team
- Solving problems that arise
- Pass work from one team member to another
- Processes and procedures for getting work done
- Determine how the team will be recognized for their efforts
- Determine how often the team should meet
Moving forward, after this initial meeting, the team leader should regularly check on progress and ensure the team keeps moving forward to meet the goals of the objectives. This may be done during team meetings but should also entail some one-on-one time with team members.
What should have been done from day one when these issues surfaced?
Had all of this been done early on when the project was first launched, the team may be in a different place. Every team needs time to get to know each other to build trust and to collaborate on how they will work together. As a best practice, I kick off every project with an initial team meeting focused on the team getting to know each other – building relationships with each other and building trust. A variety of team activities can help accomplish this.
Comments are closed.
Purchase Your Copy Today!

| The opinions expressed in this blog are my own and don’t represent the views of my current or former employers. These postings should be considered as guidance and “food for thought” but not professional advice. |
| Copyright © 2009 - 2024 - All Rights Reserved - |
Session 2. Teamwork and Communication in Health Care

Chapter 6. Case-Based Learning
At a glance.
| Teamwork and Communication in Health Care | |
| Pharmacy, Nursing, Speech-Language Pathology and Audiology | |
| Clinical skills | |
| Domain: Teams and Teamwork Describe the process of team development and the roles and practices of effective teams. Reflect on individual and team performance for individual, as well as team, performance improvement. | |
| Domain: Interprofessional Collaborative Practice Exchange meaningful information among health care providers to identify and implement appropriate, high quality care for patients, based on comprehensive evaluations and options available within the local health delivery and referral system. | |
| Understand the terminology and concepts of interprofessional education and collaborative practice. Consider how collaborative practice can increase provision of comprehensive oral health services. |
Instructor’s Guide
Overview for instructors. The purpose of this didactic session is to introduce students to the concepts of interprofessional education and collaborative practice. Instructors will use two case studies to highlight the specific teamwork and communication skills individuals need to work effectively on an interprofessional health care team. Each case study uses little to no medical or dental terminology to embed oral health. As a result, this session is ideal for pre-licensure health sciences students with no clinical training.
Materials provided in this toolkit.
- Pre- and Post-Session Assessment Questionnaire
- Instructor’s Copy, Case Study: Jill
- Instructor’s Copy, Case Study: Mr. Jones
- Case Study: Jill
- Case Study: Mr. Jones
Instructor Preparation.
- Download slides 30–34 and the accompanying speaker notes from Smiles for Life Course 1: The Relationship of Oral to Systemic Health
Note: You must register as an educator before you can download individual slides and speaker notes. Slide numbers viewed through the web interface for Smiles for Life differ from the numbers on the downloaded slides. Slide numbers in this toolkit correspond to slides in the third edition of Smiles for Life in their downloaded format.
- Ask a faculty member from each of the participating programs to locate or draft a short description of the roles and responsibilities for his or her respective profession. Compile these descriptions into one Word document and make it available to your students through email, your preferred learning management system, or your website.
- Pre-Session Assignment: Teamwork and Communication in Health Care
Note : The survey portion of the Pre- and Post-Session Assessment Questionnaire is taken from the TeamSTEPPS ® Teamwork Attitudes Questionnaire , which looks at five core components of teamwork. TeamSTEPPS was developed jointly by the Department of Defense and the Agency for Healthcare Research and Quality to improve the quality and safety of patient care. To learn more about the system, which includes a full curriculum and other resources, visit TeamSTEPPS .
- Complete the Pre- and Post-Session Assignment: Teamwork and Communication in Health Care .
- Review the roles and responsibilities document provided by the instructor.
- Pre-assessment (2–5 minutes)
- Introduction (5 minutes)
- Discussion of the pre-session assignment (10 minutes)
- Smiles for Life Course 1: The Relationship of Oral to Systemic Health PowerPoint slides 30–34 (10 minutes)
- Case study for Jill (10 minutes)
- Case study for Mr. Jones (10 minutes)
- Wrap-up (5 minutes)
- Post-assessment (2–5 minutes)
Instructor’s Notes
This session will take approximately one hour, depending on the number of participants.
Pre-assessment (2–5 minutes). Ask students to complete the pre-session portion of the Pre- and Post-Session Assessment Questionnaire as they arrive.
Introduction (5 minutes). Review the learning objectives and purpose of the session. Ask students to identify themselves by hand as you note the professions represented in class. Then, ask a student volunteer from each profession to read the roles and responsibilities for his or her profession aloud.
Discussion of pre-session assignment (10 minutes). The purpose of this assignment is to provide students with a real-world example of substandard health care delivery.
Ask student volunteers to share their answers to the questions in the Pre-Session Assignment: Teamwork and Communication in Health Care . Use the following notes to enhance discussion for each question.
- The purpose of this question is to prompt students to think about their personal experiences with teamwork. Allow a few students to share their answers.
- The purpose of this question is to prompt students to identify specific examples of effective or ineffective teamwork.
- This question should prompt students to reflect on the consequences of poor health care delivery (i.e., what happens when teamwork, collaboration, and good communication are absent).
- This question asks students to contemplate what went wrong with Deamonte’s health care delivery.
If necessary, guide students toward an understanding of the ways better communication and teamwork could have resulted in the more timely care needed to save Deamonte’s life.
Smiles for Life Course 1: The Relationship of Oral to Systemic Health PowerPoint slides 30–34 (10 minutes). This portion of Smiles for Life Course 1: The Relationship of Oral to Systemic Health introduces the concepts of interprofessional education and collaborative practice. Take time to read the definition of each and point out that the purpose of this didactic session is to prepare students for collaborative practice.
Case study for Jill (10 minutes). Break students into interprofessional teams of five or six. If possible, place one student from each profession on each team.
Instruct students to read Jill’s case study silently, then answer the questions as a team. One student should take notes and be prepared to discuss the team’s answers.
Use the following notes to enhance discussion generated by the questions.
- Yes. Although Jill’s school nurse could have taken action earlier, the dentist, physician, and school nurse communicated in a positive manner that reflects collaborative practice.
- Yes. All U.S. states and territories have laws that mandate the reporting of suspected abuse by specified individuals. These typically include physicians, nurses, and other health professionals. The need to be alert to nonmedical issues also highlights a potentially overlooked aspect of patient-centered care delivery. All health care providers should be concerned about a patient’s overall health and wellbeing, including those conditions whose treatment extends beyond the provider’s training.
- Jill’s health care team exhibited effective communication, mutual respect, and concern for comprehensive care.
- The physician addressed Jill’s oral health concerns and provided a dental referral. This illustrates patient-centered, comprehensive care.
- The dentist followed up with Jill’s physician and also consulted with her school nurse. This illustrates effective communication and collaboration.
- Participate in interprofessional education opportunities such as this one.
- Learn about the roles and responsibilities of other health care providers.
- Contact local health care providers once in practice to facilitate collaboration.
Case study for Mr. Jones (10 minutes).
Option 1 Ask students to form new teams with at least one person from each profession present on each team. Teams should designate one person to take notes and report on team findings. After the students have formed teams, direct them to read the case study for Mr. Jones silently, then answer the questions as a team.
Option 2 Ask students to remain with their present teams but designate a new person to take notes and report findings. Direct students to read the case study for Mr. Jones silently, then answer the questions as a team.
- The primary care provider (PCP) prescribed oral medication—a poor choice for patients with difficulty swallowing—and failed to refer Mr. Jones to a dentist for further evaluation.
- The speech language pathologist (SLP) did not perform an adequate oral examination, even after noticing Mr. Jones’s bad breath and food accumulation.
- The pharmacist filled the prescription for oral antibiotics in pill form without questioning the patient’s ability to swallow, even though the pharmacist recognized his facial paralysis and difficulty speaking.
- Mr. Jones’s health care team members did not communicate or collaborate with one another regarding his health care delivery.
- The PCP could have spoken to the SLP over the phone and explained that he prescribed Mr. Jones antibiotics and pain medication for an infected tooth. This may have prompted the SLP to point out the need for liquid antibiotics to ensure patient compliance. It may also have prompted the SLP to follow up with Mr. Jones regarding his oral condition at his appointment.
- Even without a call from the PCP, the SLP could have performed a comprehensive oral examination as part of Mr. Jones’s appointment and noted the infected tooth, which should have prompted an immediate dental referral.
- The pharmacist could have questioned Mr. Jones about his facial paralysis and ability to swallow. This would have prompted a change in prescription from pill to liquid form, enabling Mr. Jones to take the oral antibiotics more easily.
- Yes, the PCP could have referred Mr. Jones to a dental provider when the oral antibiotics were prescribed.
- Yes, cost and unnecessary pain and stress for the patient.
Wrap-up (5 minutes).
To facilitate a wrap-up discussion, ask students the following questions.
- Did working with students from other professions highlight aspects of health care delivery that you had not considered before?
- How will you apply what you learned today about teamwork and communication in health care to your education and in practice?
To close the session, summarize the following points for your students.
- Patient-centered health care requires all health care providers to communicate and collaborate effectively.
- A lack of communication and teamwork has been shown to negatively impact patient health outcomes.
- Patient health and safety is at risk when health care providers do not work together.
Post-assessment (2–5 minutes). Ask students to complete the post-session portion of the Pre- and Post-Session Assessment Questionnaire before they leave. Impress upon them the value of their feedback in helping you hone the session for future students.
< Previous Page: Session 1. Team-Based Care
First Published: 10/2015 Last updated: 03/2016
Next Page: Chapter 6 Resources >
- India Today
- Business Today
- Harper's Bazaar
- Brides Today
- Cosmopolitan
- India Today Hindi
- Reader’s Digest
- Aaj Tak Campus
Download App

Kolkata rape-murder case LIVE: Court allows polygraph test of RG Kar ex-principal, 4 other doctors

Court allows polygraph test of RG Kar ex-principal, 4 other doctors
A Kolkata court gave approval to the CBI to conduct a polygraph test on Dr Sandip Ghosh, the ex-principal of Kolkata's RG Kar hospital where a 31-year-old trainee doctor was raped and murdered.
The court also approved polygraph test of four other doctors, who were colleagues of the victim. They were with her on the night of crime.
Next hearing in the case to be on September 5
Kolkata Doctor Rape-Murder Case: The next hearing in the case would be on September 5. The Supreme Court asked states and UTs not to take any coercive action against doctors, who participated in protests against the doctor's rape and murder.
Supreme Court also asked the Union health secretary to hold a meeting with the chief secretaries and police chiefs of states and UTs within a week for putting in place a mechanism to ensure safety of medical professionals in public hospitals.
Supreme Court directs CBI court to pass order on polygraph test by tomorrow 5 pm
CJI: Case status report has been submitted by CBI and status report filed by Kolkata police. The investigation dealing with the death- Kolkata police is looking after the vandalism after the protest at the hospital. Polygraph test request has been submitted to the SCJM and it is under process. He shall pass order not later than 23 August 5 pm
Chief Justice questions 14-hour delay in registering case
CJI: What is the reason (a) for FIR to be lodged 14 hours of delay; (b) the principal of the college should have supposed to come straight to the college and filed the FIR, whom is he protecting ? (c) he had resigned and assigned another college?
CBI confirms involvement of Sanjoy Roy via DNA match
The CBI, during the hearing in Supreme Court, confirmed the involvemnet of Sanjoy Roy via DNA match.
Supreme Court debunks 151 gm semen theory, Chief Justice says ‘don’t use social media arguments’
The Supreme Court debunked 151 gm semen theory during the hearing into the rape and murder case of Kolkata trainee doctor at RG Kar medical college.
On 150 gm of "semen" found -- CJI tells lawyer "please don't use social media to make your arguments"
CJI: We have the PM report, and we know what that 151 refers to.
Supreme Court slams Kolkata police, questions sealing crime scene delay
The Supreme Court, during the hearing into the Kolkata trainee doctor rape and murder, slammed the Kolkata police and questioned the delay in sealing the crime scene.
"Why was the crime scene sealed after 18 hours of autopsy?," the Supreme Court questioned the cops.
Calcutta High Court declines to issue gag order in medical college ex-principal’s plea alleging media trial
The Calcutta High Court has refused to issue an order restraining media outlets from broadcasting news about former RG Kar principal Dr Sandip Ghosh.
Kolkata doctor rape case: Very surprising, post-mortem precedes registration of unnatural death: Supreme Court
Justice JB Pardiwala: When you start performing the post mortem, it means that its case of unnatural death, UD 861/24 was registered at 11:20 pm, 9th August the GD entry and FIR recorded at 11:45 pm, is this true? This is very surprising, post mortem precedes registration of the unnatural death!
Crime scene at RG Kar was altered, says CBI in Supreme Court
The CBI, during a hearing into the Kolkata rape-murder case in Supreme Court, said that the crime scene at the RG Kar Medical College was altered.
Family was misled saying suicide, crime scene altered: Solicitor General for Centre
Solicitor General Tushar Mehta, representing for Centre, said that the victim's family was misled by saying their daughter had committed suicide. Also, the crime scene was altered, the Solicitor General said in the Supreme Court.
Supreme Court bench reads CBI report
The Supreme Court bench reads the status report submitted by the CBI.
Not just about rape-murder, Dr Ghosh did financial scams, says doctors’ counsel
The doctors' counsel, during the Supreme Court hearing, said that the case is not just about the rape-murder of the trainee doctor but about financial fraud too. Ex-principal of RG Kar medical college, Sandip Ghosh, did financial scams, said doctors’ counsel.
I have personally slept on the floor of a public hospital, says CJI
The Chief Justice said that he is concerned over doctors’ working hours. “Please assure the doctors that we know they are working for 36 hours. I have personally slept on the floor of a public hospital when one my family member was not well,” said the Chief Justice.
Supreme Court begins hearing, Chief Justice asks doctors to return to work
The Chief Justice of India asked the protesting doctors to return to work and assured that the task force will take care of them. He also said that no action should be taken on the protesting doctors returning to work.
Chief Justice to doctors: They should work. They should return to work. None will take any action against the doctors. We understand they were upset but first let them report to work.
No adverse action should be taken against doctors returning to work, said the Chief Justice.
Unequal battle, says BJP’s Amit Malviya as 21-member legal team represents Bengal government
As a team of 21 advocates are representing the Bengal government in the Supreme Court in the Kolkata trainee doctor rape-murder case, BJP MP Amit Banerjee called it an “unequal battle”.
He said, “What is Mamata Banerjee trying to hide in the RG Kar Medical College & Hospital rape and murder case? 21 lawyers, led by former Congressman Kapil Sibal, are representing the Bengal Govt, which stands accused of ‘abuse of power’.”
He added, “Imagine: on the one side is an average middle class family living in the suburbs of Kolkata, whose daughter dreamt of becoming a doctor and serving the people, and on the other hand is a coalition of the corrupt and powerful. It is an unequal battle. But the people of West Bengal will triumph, no matter what.”
TMC MP Abhishek Banerjee calls for anti-rape law
TMC MP Abhishek Banerjee called for an anti-rape law as the Supreme Court is scheduled to hear the Kolkata trainee doctor rape and murder case shortly.
In a post on X, the Trinamool MP said, “We need strong laws that mandate trials and convictions within 50 days, followed by the severest punishments, not just empty promises. State governments must act and urgently push the Union for a comprehensive anti-rape law that ensures swift and strict justice. Anything less is merely symbolic and tragically ineffective.”
Congress leader Sachin Pilot says ‘example-setting punishment’ must be given to accused
Kolkata doctor rape-murder: In a recent interview, senior Congress leader Sachin Pilot expressed deep concern over the horrific rape and murder of a doctor in Kolkata. Describing the incident as heart-wrenching, Pilot empathised with the anger and frustration felt by the medical community.
"This was a gut-wrenching incident. We can understand the anger of the doctors," Pilot said. He emphasized the need for exemplary punishment for the accused to ensure such crimes find no place in society. "An example-setting punishment must be given to the perpetrator. There is no place for such incidents in our society," he added.
Pilot also questioned, "If such crimes continue to happen to our sisters and daughters, what progress are we even talking about?", urging immediate and stringent action to prevent such heinous acts in the future.
Video: Ex-principal of RG Kar Medical College arrives at CBI office
The former principal of RG Kar Medical College and Hospital, Sandip Ghosh, arrived at CBI office, in connection with ongoing probe into woman doctor rape and murder case.
#WATCH | West Bengal: Former principal of RG Kar Medical College and Hospital, Sandip Ghosh arrives at CBI office, in connection with ongoing probe into woman doctor rape and murder case. pic.twitter.com/CQ86JETr23 — ANI (@ANI) August 22, 2024
Kolkata rape murder case: CBI to resume hearing shortly
The Supreme Court will resume the hearing into the rape and murder case of the Kolkata trainee doctor at RG Kar Medical College. A bench led by Chief Justice of India DY Chandrachud and comprising Justices JB Pardiwala and Manoj Mishra heard the case on Tuesday (August 20). It had asked for status reports on the probe into the rape-murder and vandalism at RG Kar hospital from the CBI and the Bengal government, respectively.

Summary. In this fictional case, the CEO of a sports apparel manufacturer is faced with an ongoing conflict between two of his top executives. Specifically, the head of sales and the CFO are at ...
Most work today is done in teams. While teamwork can lead to innovative ideas and strong performance, it can also be stressful. Conflicts arise, people become too dependent on each other, some don ...
Develop processes and procedures for how the team will: share work, meet the objectives of the project, solve problems and resolve conflicts and make decisions. When the team members get to know each other, they will begin to support each other and will be more concerned about their team mates. Bottom line, they will function as a team.
Clarify task and role expectations. When everyone assumes that someone else is responsible for completing a task, balls are inevitably dropped, leading to finger-pointing, blame, and missed ...
Teamwork is essential for success no matter what industry you're in, but it can be derailed in a number of different ways. Connecting the dots between what your team is doing and why they're doing it goes a long way in addressing (and preventing) many of the most common teamwork challenges.; Taking the time to listen to team members' hopes and concerns builds a better working ...
Teamwork can have great benefits, but several predictable challenges can negatively impact team performance. In this paper, we examine these challenges, and summarize nine of the most common barriers to effective teamwork (i.e., competing demands, undervaluing teammates, power differentials, a leader not promoting collaboration, inexperience ...
A case study is used to investigate two teams of final year multimedia students completing a project-based unit, in which teamwork was an essential ingredient and immersed in an authentic context ...
Dan Ilgen and I began our Psychological Science in the Public Interest (PSPI) article, which was a comprehensive review of the team effectiveness literature, by noting that "teams of people working together for a common purpose have been a centerpiece of human social organization ever since our ancient ancestors first banded together to hunt game, raise families, and defend their communities ...
The science of teamwork has been extensively studied, 1 and with good reason. Successful teams improve business outcomes, including revenue and performance. 2 Many organizations are intentionally fostering a collaborative team-based culture, 2 and feeling like a part of a team is a primary driver of employee engagement. 3 Prior to the pandemic, organizational shifts had resulted in teams that ...
Free download. 👉 TL;DR. Good team dynamics include open communication, clear expectations, and mutual trust, leading to increased productivity and employee satisfaction. In contrast, bad team dynamics involve poor communication, unresolved conflicts, and a lack of collaboration, resulting in decreased efficiency and higher employee turnover.
A set of common teamwork challenges were identified using the survey and qualitative data. Qualitative data was analyzed to explore the unique ways these challenges manifest in both clinical and ...
Contextual factors of teamwork effectiveness. Based on a large body of team research from various domains, we hypothesise that several contextual and methodological factors might moderate the effectiveness of teamwork, indicating that teamwork is more important under certain conditions. 31 32 Therefore, we investigate several factors: (a) team characteristics (ie, professional composition ...
There are various barriers that teams may face when working together. Here are 11 of the most common impediments to teamwork that groups of professionals face, including strategies for overcoming them: 1. Ineffective leadership. For teams to work together effectively, they need leaders who can guide them, offer their insight and encourage ...
Among co-workers, it appears easier to learn bad behavior than good. A recent study has found that financial advisors are 37% more likely to commit misconduct if they encounter a new co-worker ...
Check out our team building case study round-up of 16 corporate teams we helped to improve morale, collaboration, and relationships. Phone 1-800-565-8735. Request a Quote. Virtual Team Building; ... Supporting teamwork in an increasingly remote and hybrid environment is no easy task. In this guest article from Erica Pezza, you'll learn 15 ...
Among the emotions discussed by participants, stress, being in a "bad mood", or feeling scared of others, were indicated as barriers to teamwork while positive emotions were viewed as enablers of effective teamwork by participants. ... This sets our work apart from other studies of OR teamwork, ... A case study of a trial of individualized ...
Introduction. Effective teamwork between healthcare professionals is recognized to be a critical element of patient safety and quality of care [].Research has consistently demonstrated that the nature of the collaboration between doctors and nurses is related to patient outcomes such as the duration of patient stay [], patient mortality [] and the occurrence of medication errors [].
Abstract. This 3-year research project assessed the effectiveness of a teambuilding intervention among a group of department leaders who supervised a fire management unit working in the forests of the western United States. The intervention began with a 3-day retreat that covered three basic areas: communication skills, consensus building, and ...
Dmitri Kara, a tenancy expert at Fantastic Cleaners, shared with us a team-building exercise his team uses to increase cooperation and efficiency. "Everybody in the office has to simultaneously perform a 2-to-5-minute cleaning routine (like wipe their desk, keyboard, monitor, shelves). But there's a catch: the tools are limited.
Martine Haas. and. Mark Mortensen. From the Magazine (June 2016) RW13 (Fair Game), oil on canvas, Museum of Fine Arts, Boston, 2010 Jeff Perrott. Summary. Over the years, as teams have grown more ...
Working with the team, the team leader should collaboratively: Set team goals (in line with the objectives of the project) Determine roles and responsibilities on the team. Determine how the team members will work together, including: Resolving conflicts on the team. Solving problems that arise. Pass work from one team member to another.
Ask students to form new teams with at least one person from each profession present on each team. Teams should designate one person to take notes and report on team findings. After the students have formed teams, direct them to read the case study for Mr. Jones silently, then answer the questions as a team. Option 2.
Abstract Healthcare professionals report poor overall well-being, with many citing mental health concerns and stress as contributing factors. ... and MPs within the selected Australian LHD. A case study design was used to understand the resource gains and resource losses during the case study organization from 2019 to 2021. ... teamwork is ...
Kolkata doctor rape murder case live updates: The Central Bureau of Investigation (CBI) has submitted a progress report on the investigation into the gruesome rape and murder of a woman trainee doctor at Kolkata's RG Kar Medical College and Hospital to the Supreme Court. A bench led by Chief Justice of India DY Chandrachud and comprising Justices JB Pardiwala and Manoj Mishra heard the case today.
- business plan
- course work
- research paper
IMAGES
VIDEO
COMMENTS
2024 Yacht-Master 42 Titanium RLX Oyster 226627 42mm Complete Set BNIB $ 27,495. Free shipping. US. Promoted. Rolex Yacht-Master 42. ... NEW Rolex Yacht-Master 42 RLX Titanium Intense Black Dial Watch B/P '24 226627 $ 29,500 + $99 for shipping. US. The Secure Path to Your Dream Watch.
Buy and sell authentic used Rolex Yacht-Master 42 watches. Explore great deals from local and international sellers on the Chrono24 marketplace. ... 2023 PAPERS Rolex Yacht-Master 226658 Yellow Gold 42mm Oysterflex Watch Box $ 30,992 + $129 for shipping. US. Promoted. ... RLX Titanium $ 34,950 + $150 for shipping. US. Rolex Yacht-Master 42 ...
The Oyster bracelet Alchemy of form and function. The Yacht-Master 42, made from RLX titanium, is fitted on an Oyster bracelet. Developed at the end of the 1930s, this three-piece link bracelet remains the most universal in the Oyster Perpetual collection and is known for its robustness.
Rolex Yacht-Master 42 Listing: $28,500 Rolex Yacht-Master 42, Reference number 226659; White gold; Automatic; Condition Very good; Year 2022; Watch with orig. ... Offering for sale this lightly worn Rolex Oyster Perptual Yachtmaster. A reference 226659, 42mm 18K white gold case, screw-down crown with triplock triple waterproofness system ...
Rolex. Yacht-Master 42 Oyster, 42 mm, RLX titanium M226627-0001. $14,050 Suggested retail price before applicable taxes. The suggested price can be modified at any time without notice. ... Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its ...
Yacht-Master 42. Oyster, 42 mm, RLX titanium. m226627-0001. $ 14,050. Rolex's suggested retail price before applicable taxes. Rolex reserves the right to change the prices at any time without notice. +16305715355.
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes - triangles, circles, rectangles - are filled with a luminescent material emitting a long-lasting glow.
M226627-0001. Model case. Oyster, 42 mm, RLX titanium. Water-resistance. Waterproof to 100 metres / 330 feet. Bezel. Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations. Dial. Intense black.
Rolex. Yacht-Master 42. Oyster, 42 mm, RLX titanium +1 954-710-5742. Message. Find us. Model availability. Reference. 226627. Model case. Oyster, 42 mm, RLX titanium. Water-resistance. Waterproof to 100 metres / 330 feet. Bezel. Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised ...
Oyster, 42 mm, RLX titanium. $14,050. ... Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. ... Rolex Yacht-Master. Marine character. Learn More . Keep Exploring. Discover Rolex. Rolex Watches. New Watches 2024. Watchmaking.
Rolex Yacht-Master 42 Listing: $32,000 Rolex Yacht-master 42, Reference number 226658; Yellow gold; Automatic; Condition Good; Year 2023; Watch with original
Intense black dial. Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes - triangles, circles, rectangles - are filled with a luminescent material emitting a long-lasting glow.
Like all Rolex Professional watches, the Yacht-Master 42 offers exceptional legibility in all circumstances, and especially in the dark, thanks to its Chromalight display. The broad hands and hour markers in simple shapes - triangles, circles, rectangles - are filled with a luminescent material emitting a long-lasting glow.
For the modern man with an eye for luxury, the Rolex Yacht-Master 42 226627-0001 is an ideal timepiece. Crafted from RLX titanium, this 42mm case offers a robust yet lightweight feel that won't weigh you down. The black dial and dot and index hour markers are complemented by a black ceramic bezel that adds a subtle splash of style.
Yacht-Master 42. Oyster, 42 mm, RLX titanium. $ 14,050. Model availability. Reference 226627. Model case Oyster, 42 mm, RLX titanium. Water-resistance Waterproof to 100 metres / 330 feet. Bezel Bidirectional rotatable 60-minute graduated bezel with matt black Cerachrom insert in ceramic, polished raised numerals and graduations.
Rolex Yacht-Master 40 Listing: £11,402 Rolex Yacht-Master, Reference number 16623; Gold/Steel; Automatic; Condition Good; Year 2007; Watch with original b. Skip. Have you tried the Chrono24 app? Discover now ! Search through 604,062 watches from 130 countries. ... + £42 for shipping. UK.
2021 NEW CARD Rolex Yacht-Master BLACK Oysterflex 42mm 18K Gold 226659 BOX $ 27,993 + $175 for shipping. US. Promoted. ... 2024 Yacht-Master 42 Titanium RLX Oyster 226627 42mm Complete Set BNIB $ 27,495. Free shipping. US. Rolex Yacht-Master 42. 226627 $ 29,900 + $50 for shipping. US. Promoted.
Shop New Arrivals. Master Chronometer vs Superlative Chronometer. Accuracy has always been an important point of pride and marketing for luxury watch brands. For over a century, t
Oyster Perpetual. Yacht-Master 42. An emblematic watch in rlx titanium. The emblematic watch of the sailing world, the Oyster Perpetual Yacht-Master 42 is now available in RLX tit
This Rolex Yacht-Master is designed with a 42mm RLX-titanium case and black dial, styled on a matching titanium Oyster bracelet. Luminous hour markers, hands, and a Chromalight display provide clear legibility in every circumstance. Complications include a bidirectional 60-minute bezel, stop-time keeping, and water resistance up to 100 meters.
Item Return Policy. Ben Bridge is committed to ensure our customers are happy with their purchase or gifts. If you have any questions or concerns about our refund policy, please c
Shop New Arrivals. Rolex Yacht-Master. Yacht-Master; Yacht-Master II; Rolex 16622; Rolex 168622; $7,000 to $10,000; $10,000 to $15,000; $15,000 to $20,000; Stainless ...
Rolex Yacht-Master 42 Listing: $35,198 Rolex Yacht-Master 42 New / Unworn with box and papers, Reference number 226659; White gold; Automatic; Condition Like new & unworn; Year 2022; Watch w
Rolex Yacht-Master 42 Listing: Price on request Rolex Yacht-Master 42 226627, Reference number 226627; Titanium; Automatic; Condition Like new & unworn; Watch with original . ... Rolex Yacht-Master 42 "Falcon Eye" 226659. Price on request + $204 for shipping. UK. Rolex Yacht-Master 42. 226659. Price on request + $204 for shipping. UK.